

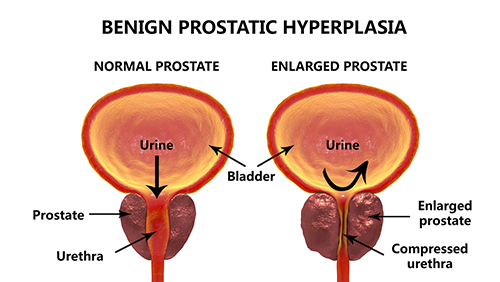
Figure 1. Normal and enlarged prostates and how they affect bladder emptying
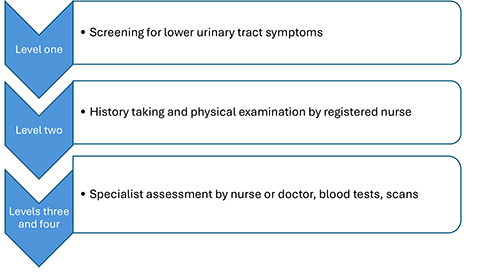
Figure 2. The screening, assessment and investigation process
References
Abrams P, Cardozo L, Fall M et al; Standardisation Sub-committee of the International Continence Society (2002) The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn. 21(2):167-78. https://doi.org/10.1002/nau.10052
Andrade M, Knight J (2017) Anatomy and physiology of ageing 4: the renal system. Nursing Times 113(5):46-49
Barry MJ, Fowler FJ Jr, O’Leary MP et al; Measurement Committee of the American Urological Association (2017) The American Urological Association symptom index for benign prostatic hyperplasia. J Urol. 197(2S):S189-S197. https://doi.org/10.1016/j.juro.2016.10.071
Bishara D (2023) Managing drugs with anticholinergic activity. Drug Ther Bull. 61(9):135-139. https://doi.org/10.1136/dtb.2022.000066
Bradley CS, Erickson BA, Messersmith EE et al; Symptoms of Lower Urinary Tract Dysfunction Research Network (LURN) (2017) Evidence of the impact of diet, fluid intake, caffeine, alcohol and tobacco on lower urinary tract symptoms: a systematic review. J Urol. 198(5):1010-1020. https://doi.org/10.1016/j.juro.2017.04.097
British National Formulary (2025) Lower urinary tract symptoms in males. https://bnf.nice.org.uk/treatment-summaries/lower-urinary-tract-symptoms-in-males (accessed 12 September 2025)
Chughtai B, Forde JC, Thomas DD et al (2016) Benign prostatic hyperplasia. Nat Rev Dis Primers. 2:16031. https://doi.org/10.1038/nrdp.2016.31
Curtin D, Gallagher P, O'Mahony D (2021) Deprescribing in older people approaching end-of-life: development and validation of STOPPFrail version 2. Age Ageing. 50(2):465-471. https://doi.org/10.1093/ageing/afaa159
Deters LA (2024) Benign prostatic hyperplasia (BPH). https://emedicine.medscape.com/article/437359-overview (accessed 12 September 2025)
Egan KB (2016) The epidemiology of benign prostatic hyperplasia associated with lower urinary tract symptoms: prevalence and incident rates. Urol Clin North Am. 43(3):289–297. https://doi.org/10.1016/j.ucl.2016.04.001
Emberton M, Marberger M, de la Rosette J (2008) Understanding patient and physician perceptions of benign prostatic hyperplasia in Europe: The Prostate Research on Behaviour and Education (PROBE) Survey. Int J Clin Pract. 62(1):18–26. https://doi.org/10.1111/j.1742-1241.2007.01635.x
Fair WR, Parrish RF (1981) Antibacterial substances in prostatic fluid. Prog Clin Biol Res. 75A:247-64.
Fusco F, Creta M, De Nunzio C et al (2018) Progressive bladder remodeling due to bladder outlet obstruction: a systematic review of morphological and molecular evidences in humans. BMC Urol. 18(1):15. https://doi.org/10.1186/s12894-018-0329-4
Gacci M, Corona G, Vignozzi L et al (2015) Metabolic syndrome and benign prostatic enlargement: a systematic review and meta-analysis. BJU Int. 115(1):24-31. https://doi.org/10.1111/bju.12728
Healthcare Improvement Scotland (2023) Red flags and serious pathology. https://rightdecisions.scot.nhs.uk/ggc-msk-index-in-development/red-flags (accessed 12 September 2025)
King R, Rabino S. ACB Calculator. https://www.acbcalc.com/medicines (accessed 12 September 2025)
Kinter KJ, Amraei R, Anekar AA (2023) Biochemistry, Dihydrotestosterone. https://www.ncbi.nlm.nih.gov/books/NBK557634/ (accessed 19 September 2025)
Lim KB (2017) Epidemiology of clinical benign prostatic hyperplasia. Asian J Urol. 4(3):148-151. https://doi.org/10.1016/j.ajur.2017.06.004
Liu HH, Tsai TH, Lee SS, Kuo YH, Hsieh T (2016) Maximum urine flow rate of less than 15ml/sec increasing risk of urine retention and prostate surgery among patients with alpha-1 blockers: a 10-year follow up study. PLoS One. 11(8):e0160689. https://doi.org/10.1371/journal.pone.0160689
Mansbart F, Kienberger G, Sönnichsen A et al (2022) Efficacy and safety of adrenergic alpha-1 receptor antagonists in older adults: a systematic review and meta-analysis supporting the development of recommendations to reduce potentially inappropriate prescribing. BMC Geriatr. 22:771. https://doi.org/10.1186/s12877-022-03415-7
Nachawati D, Leslie SW, Patel JB (2025) Alpha-blockers. https://www.ncbi.nlm.nih.gov/books/NBK556066/ (accessed 12 September 2025)
National Institute for Health and Care Excellence (2024) Lower urinary tract symptoms in men: recommendations [CG97]. https://www.nice.org.uk/Guidance/CG97 (accessed 12 September 2025)
National Institute for Health and Care Excellence (2025) Lower urinary tract symptoms in men. https://cks.nice.org.uk/topics/luts-in-men/ (accessed 12 September 2025)
Ng M, Leslie SW, Baradhi KM (2024) Benign prostatic hyperplasia. https://www.ncbi.nlm.nih.gov/books/NBK558920/ (accessed 12 September 2025)
Nickel JC, Gilling P, Tammela TL et al (2011) Comparison of dutasteride and finasteride for treating benign prostatic hyperplasia: the Enlarged Prostate International Comparator Study (EPICS). BJU Int. 108:388–94. https://doi.org/10.1111/j.1464-410x.2011.10195.x
Nygård LH, Talala K, Taari K, Tammela TLJ, Auvinen A, Murtola TJ (2023) Antidiabetic drugs, glycemic control and risk of benign prostatic hyperplasia. Prostate. 83(3):246-258. https://doi.org/10.1002/pros.24456
O’Mahony D, O’Sullivan D, Byrne S, O'Connor MN, Ryan C, Gallagher P (2015) STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing. 44(2):213-8. https://doi.org/10.1093/ageing/afu145
Ramanayake RPJC, Basnayake BMTK (2018) Evaluation of red flags minimizes missing serious diseases in primary care. J Family Med Prim Care. 7:315. https://doi.org/10.4103/jfmpc.jfmpc_510_15
Roehrborn CG (2008) Pathology of benign prostatic hyperplasia. Int J Impot Res. 20 Suppl 3:S11-8. https://doi.org/10.1038/ijir.2008.55
Roehrborn CG, Bruskewitz R, Nickel JC et al; Proscar Long-Term Efficacy and Safety Study Group (2004) Sustained decrease in incidence of acute urinary retention and surgery with finasteride for 6 years in men with benign prostatic hyperplasia. J Urol. 171(3):1194-8. https://doi.org/10.1097/01.ju.0000112918.74410.94
Speakman M, Kirby R, Doyle S, Ioannou C (2015) Burden of male lower urinary tract symptoms (LUTS) suggestive of benign prostatic hyperplasia (BPH) - focus on the UK. BJU Int. 115(4):508-19. https://doi.org/10.1111/bju.12745
UK Parliament (2009) Treatment for prostate diseases. https://edm.parliament.uk/early-day-motion/39704/treatment-for-prostate-diseases (accessed 12 September 2025)
Wiedemer J, McCoy T, Yu M (2021) Benign prostatic hyperplasia in African American men merits greater consideration in academic medicine. Annals of Advanced Medical Science. 4(2):000164. https://doi.org/10.23880/aabsc-16000164
Yang DY, Lee WK (2019) A current perspective on post-micturition dribble in males. Investig Clin Urol. 60(3):142-147. https://doi.org/10.4111/icu.2019.60.3.142
Yeboah E (2016) Prevalence of benign prostatic hyperplasia and prostate cancer in Africans and Africans in the diaspora. J West Afr Coll Surg. 6:1–30
Andrade M, Knight J (2017) Anatomy and physiology of ageing 4: the renal system. Nursing Times 113(5):46-49
Barry MJ, Fowler FJ Jr, O’Leary MP et al; Measurement Committee of the American Urological Association (2017) The American Urological Association symptom index for benign prostatic hyperplasia. J Urol. 197(2S):S189-S197. https://doi.org/10.1016/j.juro.2016.10.071
Bishara D (2023) Managing drugs with anticholinergic activity. Drug Ther Bull. 61(9):135-139. https://doi.org/10.1136/dtb.2022.000066
Bradley CS, Erickson BA, Messersmith EE et al; Symptoms of Lower Urinary Tract Dysfunction Research Network (LURN) (2017) Evidence of the impact of diet, fluid intake, caffeine, alcohol and tobacco on lower urinary tract symptoms: a systematic review. J Urol. 198(5):1010-1020. https://doi.org/10.1016/j.juro.2017.04.097
British National Formulary (2025) Lower urinary tract symptoms in males. https://bnf.nice.org.uk/treatment-summaries/lower-urinary-tract-symptoms-in-males (accessed 12 September 2025)
Chughtai B, Forde JC, Thomas DD et al (2016) Benign prostatic hyperplasia. Nat Rev Dis Primers. 2:16031. https://doi.org/10.1038/nrdp.2016.31
Curtin D, Gallagher P, O'Mahony D (2021) Deprescribing in older people approaching end-of-life: development and validation of STOPPFrail version 2. Age Ageing. 50(2):465-471. https://doi.org/10.1093/ageing/afaa159
Deters LA (2024) Benign prostatic hyperplasia (BPH). https://emedicine.medscape.com/article/437359-overview (accessed 12 September 2025)
Egan KB (2016) The epidemiology of benign prostatic hyperplasia associated with lower urinary tract symptoms: prevalence and incident rates. Urol Clin North Am. 43(3):289–297. https://doi.org/10.1016/j.ucl.2016.04.001
Emberton M, Marberger M, de la Rosette J (2008) Understanding patient and physician perceptions of benign prostatic hyperplasia in Europe: The Prostate Research on Behaviour and Education (PROBE) Survey. Int J Clin Pract. 62(1):18–26. https://doi.org/10.1111/j.1742-1241.2007.01635.x
Fair WR, Parrish RF (1981) Antibacterial substances in prostatic fluid. Prog Clin Biol Res. 75A:247-64.
Fusco F, Creta M, De Nunzio C et al (2018) Progressive bladder remodeling due to bladder outlet obstruction: a systematic review of morphological and molecular evidences in humans. BMC Urol. 18(1):15. https://doi.org/10.1186/s12894-018-0329-4
Gacci M, Corona G, Vignozzi L et al (2015) Metabolic syndrome and benign prostatic enlargement: a systematic review and meta-analysis. BJU Int. 115(1):24-31. https://doi.org/10.1111/bju.12728
Healthcare Improvement Scotland (2023) Red flags and serious pathology. https://rightdecisions.scot.nhs.uk/ggc-msk-index-in-development/red-flags (accessed 12 September 2025)
King R, Rabino S. ACB Calculator. https://www.acbcalc.com/medicines (accessed 12 September 2025)
Kinter KJ, Amraei R, Anekar AA (2023) Biochemistry, Dihydrotestosterone. https://www.ncbi.nlm.nih.gov/books/NBK557634/ (accessed 19 September 2025)
Lim KB (2017) Epidemiology of clinical benign prostatic hyperplasia. Asian J Urol. 4(3):148-151. https://doi.org/10.1016/j.ajur.2017.06.004
Liu HH, Tsai TH, Lee SS, Kuo YH, Hsieh T (2016) Maximum urine flow rate of less than 15ml/sec increasing risk of urine retention and prostate surgery among patients with alpha-1 blockers: a 10-year follow up study. PLoS One. 11(8):e0160689. https://doi.org/10.1371/journal.pone.0160689
Mansbart F, Kienberger G, Sönnichsen A et al (2022) Efficacy and safety of adrenergic alpha-1 receptor antagonists in older adults: a systematic review and meta-analysis supporting the development of recommendations to reduce potentially inappropriate prescribing. BMC Geriatr. 22:771. https://doi.org/10.1186/s12877-022-03415-7
Nachawati D, Leslie SW, Patel JB (2025) Alpha-blockers. https://www.ncbi.nlm.nih.gov/books/NBK556066/ (accessed 12 September 2025)
National Institute for Health and Care Excellence (2024) Lower urinary tract symptoms in men: recommendations [CG97]. https://www.nice.org.uk/Guidance/CG97 (accessed 12 September 2025)
National Institute for Health and Care Excellence (2025) Lower urinary tract symptoms in men. https://cks.nice.org.uk/topics/luts-in-men/ (accessed 12 September 2025)
Ng M, Leslie SW, Baradhi KM (2024) Benign prostatic hyperplasia. https://www.ncbi.nlm.nih.gov/books/NBK558920/ (accessed 12 September 2025)
Nickel JC, Gilling P, Tammela TL et al (2011) Comparison of dutasteride and finasteride for treating benign prostatic hyperplasia: the Enlarged Prostate International Comparator Study (EPICS). BJU Int. 108:388–94. https://doi.org/10.1111/j.1464-410x.2011.10195.x
Nygård LH, Talala K, Taari K, Tammela TLJ, Auvinen A, Murtola TJ (2023) Antidiabetic drugs, glycemic control and risk of benign prostatic hyperplasia. Prostate. 83(3):246-258. https://doi.org/10.1002/pros.24456
O’Mahony D, O’Sullivan D, Byrne S, O'Connor MN, Ryan C, Gallagher P (2015) STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing. 44(2):213-8. https://doi.org/10.1093/ageing/afu145
Ramanayake RPJC, Basnayake BMTK (2018) Evaluation of red flags minimizes missing serious diseases in primary care. J Family Med Prim Care. 7:315. https://doi.org/10.4103/jfmpc.jfmpc_510_15
Roehrborn CG (2008) Pathology of benign prostatic hyperplasia. Int J Impot Res. 20 Suppl 3:S11-8. https://doi.org/10.1038/ijir.2008.55
Roehrborn CG, Bruskewitz R, Nickel JC et al; Proscar Long-Term Efficacy and Safety Study Group (2004) Sustained decrease in incidence of acute urinary retention and surgery with finasteride for 6 years in men with benign prostatic hyperplasia. J Urol. 171(3):1194-8. https://doi.org/10.1097/01.ju.0000112918.74410.94
Speakman M, Kirby R, Doyle S, Ioannou C (2015) Burden of male lower urinary tract symptoms (LUTS) suggestive of benign prostatic hyperplasia (BPH) - focus on the UK. BJU Int. 115(4):508-19. https://doi.org/10.1111/bju.12745
UK Parliament (2009) Treatment for prostate diseases. https://edm.parliament.uk/early-day-motion/39704/treatment-for-prostate-diseases (accessed 12 September 2025)
Wiedemer J, McCoy T, Yu M (2021) Benign prostatic hyperplasia in African American men merits greater consideration in academic medicine. Annals of Advanced Medical Science. 4(2):000164. https://doi.org/10.23880/aabsc-16000164
Yang DY, Lee WK (2019) A current perspective on post-micturition dribble in males. Investig Clin Urol. 60(3):142-147. https://doi.org/10.4111/icu.2019.60.3.142
Yeboah E (2016) Prevalence of benign prostatic hyperplasia and prostate cancer in Africans and Africans in the diaspora. J West Afr Coll Surg. 6:1–30