

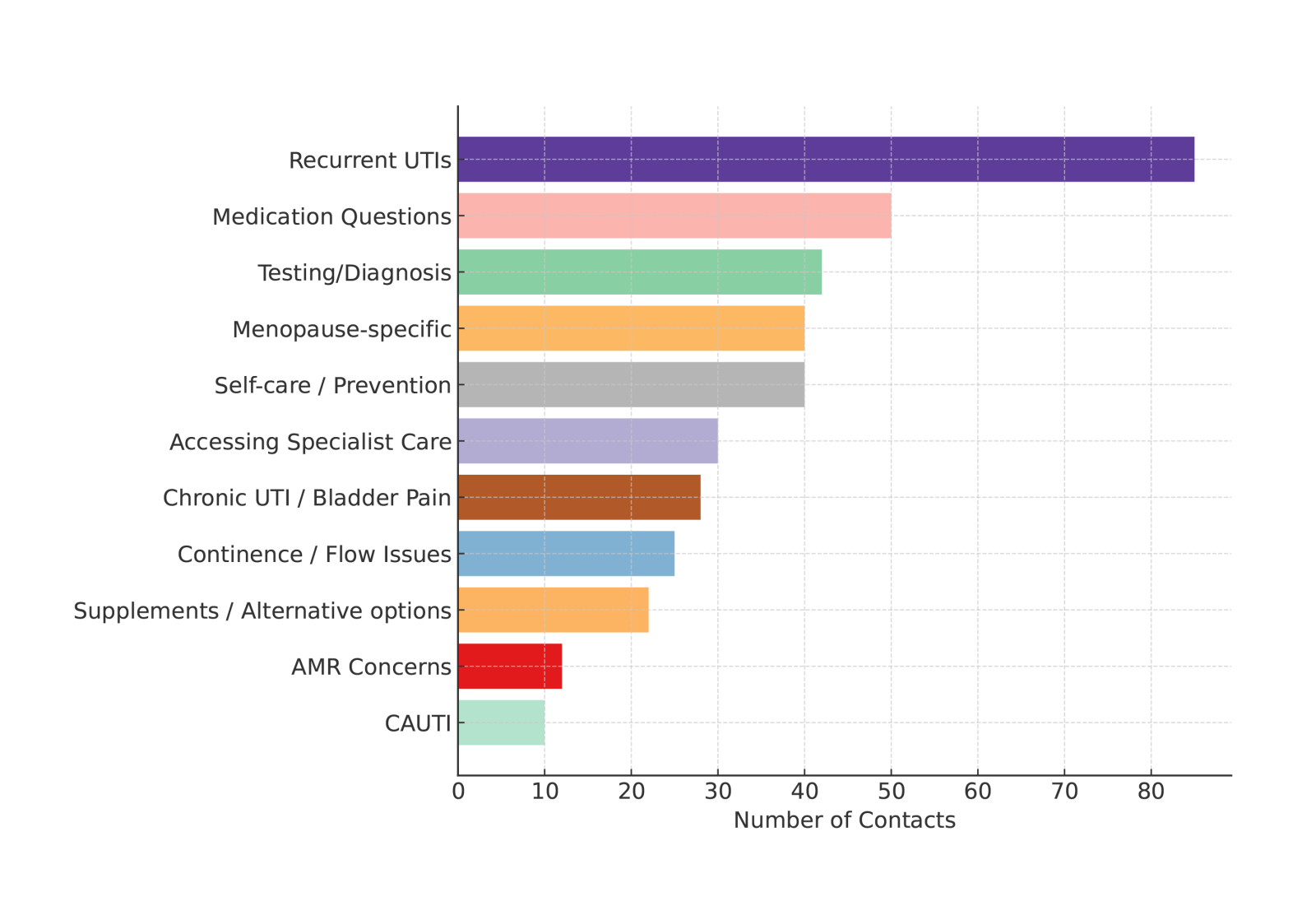
Figure 1. Most common themes of contacts with the UTI Information Service (May 2024–May 2025). AMR = antimicrobial resistance; CAUTI = catheter-associated urinary tract infection; UTI = urinary tract infection.
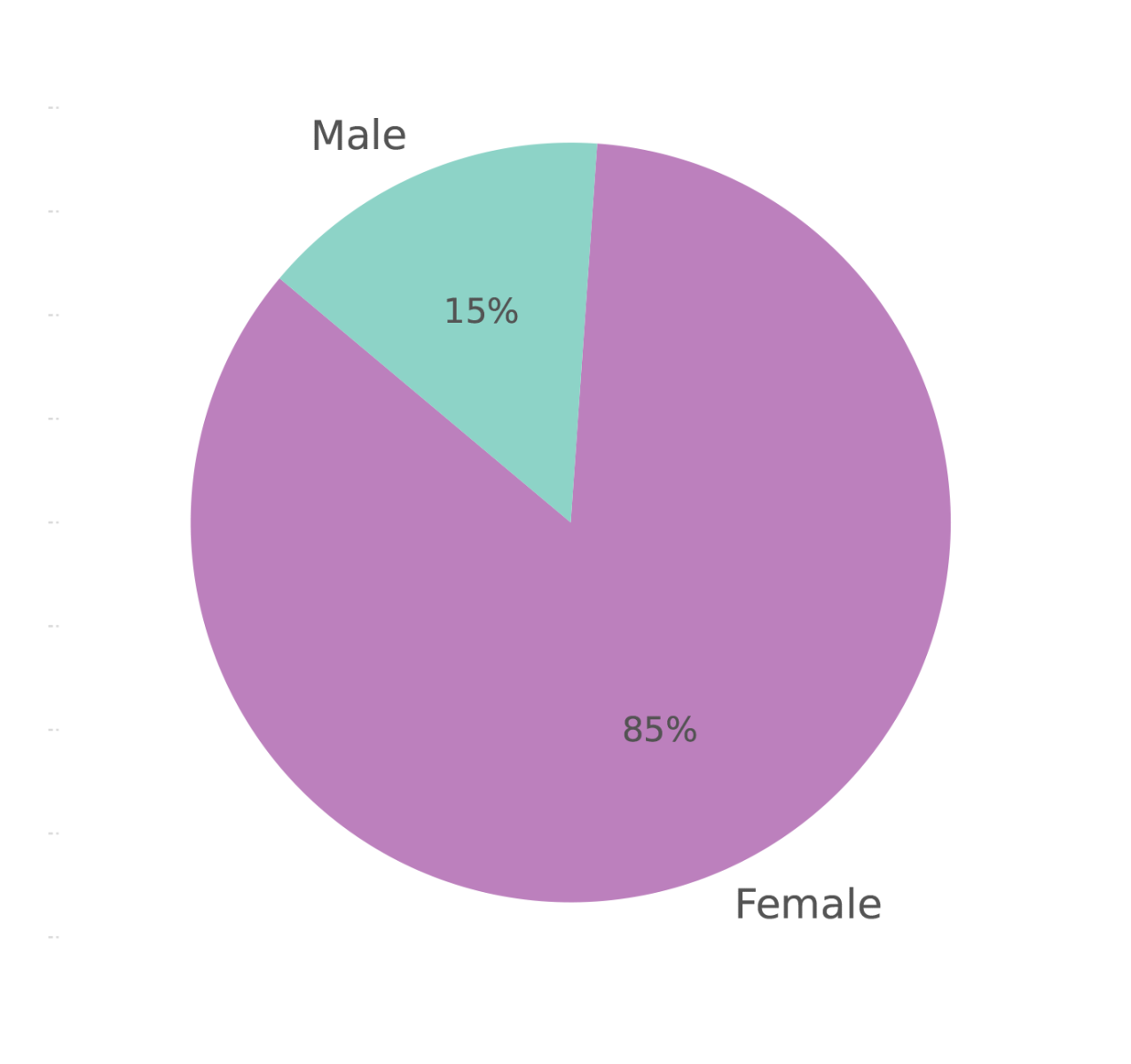
Figure 2. Gender distribution of contacts with the UTI Information Service (May 2024–May 2025).
References
Anger JT, Bixler BR, Holmes RS, Lee UJ, Santiago-Lastra Y, Selph SS (2022) Updates to Recurrent Uncomplicated Urinary Tract Infections in Women: AUA/CUA/SUFU Guideline. J Urol. 208(3):536-541. https://doi.org/10.1097/JU.0000000000002860
European Association of Urology (2025) EAU guidelines on urological infections. https://uroweb.org/guidelines/urological-infections (accessed 13 February 2026)
Foxman B (2014) Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect Dis Clin North Am. 28(1):1-13. https://doi.org/10.1016/j.idc.2013.09.003
Helplines Partnership (2024) Helplines standards. https://www.helplines.org/helplines-standard/ (accessed 13 February 2026)
James Lind Alliance (2026) Chronic and recurrent urinary tract infection (UTI). https://www.jla.nihr.ac.uk/priority-setting-partnerships/chronic-and-recurrent-urinary-tract-infection-uti (accessed 13 February 2026)
National Institute for Health and Care Excellence (2018) Urinary tract infection (lower): antimicrobial prescribing (NG109). https://www.nice.org.uk/guidance/ng109 (accessed 6 February 2026)
National Institute for Health and Care Excellence (2023) Shared decision making (NG197). https://www.nice.org.uk/guidance/ng197 (accessed 6 February 2026)
National Institute for Health and Care Excellence (2025a) Suspected sepsis in people aged 16 or over: recognition, assessment and early management (NG253). https://www.nice.org.uk/guidance/ng253 (accessed 6 February 2026)
National Institute for Health and Care Excellence (2025b) Suspected cancer: recognition and referral (NG12). https://www.nice.org.uk/guidance/ng12 (accessed 13 February 2026)
National Institute for Health and Care Research (2024) 24/69 Improving diagnosis of Urinary Tract Infection in older adults commissioning brief. https://www.nihr.ac.uk/2469-improving-diagnosis-urinary-tract-infection-older-adults-commissioning-brief (accessed 13 February 2026)
Newlands AF, Kramer M, Roberts L, Maxwell K, Price JL, Finlay KA (2024) Evaluating the quality of life impact of recurrent urinary tract infection: Validation and refinement of the Recurrent UTI Impact Questionnaire (RUTIIQ). Neurourol Urodyn. 43(4):902-914. https://doi.org/10.1002/nau.25426
The Urology Foundation (2024) The UTI Information Service and Helpline. https://www.theurologyfoundation.org/urology-health/uti-information-service-and-helpline/ (accessed 6 February 2026)
Further reading
Chen YY, Su TH, Lau HH (2021) Estrogen for the prevention of recurrent urinary tract infections in postmenopausal women: a meta-analysis of randomized controlled trials. Int Urogynecol J. 32(1):17-25. https://doi.org/10.1007/s00192-020-04397-z
Harding C, Mossop H, Homer T et al (2022) Alternative to prophylactic antibiotics for the treatment of recurrent urinary tract infections in women: multicentre, open label, randomised, non-inferiority trial. BMJ. 376:e068229. https://doi.org/10.1136/bmj-2021-0068229
National Institute for Health and Care Excellence (2018) Urinary tract infection (catheter associated): antimicrobial prescribing. https://www.nice.org.uk/guidance/ng113 (accessed 13 February 2026)
National Institute for Health and Care Excellence (2023) Urinary tract infections in adults (QS90). https://www.nice.org.uk/guidance/qs90 (accessed 13 February 2026)
National Institute for Health and Care Excellence (2024) Urinary tract infection (recurrent): antimicrobial prescribing (NG112). https://www.nice.org.uk/guidance/ng112 (accessed 13 February 2026)
National Institute for Health and Care Excellence (2025a) Urinary tract infection (lower) - men. https://cks.nice.org.uk/topics/urinary-tract-infection-lower-men/ (accessed 13 February 2026)
National Institute for Health and Care Excellence (2025b) Urinary tract infection (lower) - women. https://cks.nice.org.uk/topics/urinary-tract-infection-lower-women/ (accessed 13 February 2026)
UK Health Security Agency, NHS England (2025) Diagnosis of urinary tract infections: quick reference tools for primary care. https://www.gov.uk/government/publications/urinary-tract-infection-diagnosis/diagnosis-of-urinary-tract-infections-quick-reference-tools-for-primary-care (accessed 6 February 2026)
European Association of Urology (2025) EAU guidelines on urological infections. https://uroweb.org/guidelines/urological-infections (accessed 13 February 2026)
Foxman B (2014) Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect Dis Clin North Am. 28(1):1-13. https://doi.org/10.1016/j.idc.2013.09.003
Helplines Partnership (2024) Helplines standards. https://www.helplines.org/helplines-standard/ (accessed 13 February 2026)
James Lind Alliance (2026) Chronic and recurrent urinary tract infection (UTI). https://www.jla.nihr.ac.uk/priority-setting-partnerships/chronic-and-recurrent-urinary-tract-infection-uti (accessed 13 February 2026)
National Institute for Health and Care Excellence (2018) Urinary tract infection (lower): antimicrobial prescribing (NG109). https://www.nice.org.uk/guidance/ng109 (accessed 6 February 2026)
National Institute for Health and Care Excellence (2023) Shared decision making (NG197). https://www.nice.org.uk/guidance/ng197 (accessed 6 February 2026)
National Institute for Health and Care Excellence (2025a) Suspected sepsis in people aged 16 or over: recognition, assessment and early management (NG253). https://www.nice.org.uk/guidance/ng253 (accessed 6 February 2026)
National Institute for Health and Care Excellence (2025b) Suspected cancer: recognition and referral (NG12). https://www.nice.org.uk/guidance/ng12 (accessed 13 February 2026)
National Institute for Health and Care Research (2024) 24/69 Improving diagnosis of Urinary Tract Infection in older adults commissioning brief. https://www.nihr.ac.uk/2469-improving-diagnosis-urinary-tract-infection-older-adults-commissioning-brief (accessed 13 February 2026)
Newlands AF, Kramer M, Roberts L, Maxwell K, Price JL, Finlay KA (2024) Evaluating the quality of life impact of recurrent urinary tract infection: Validation and refinement of the Recurrent UTI Impact Questionnaire (RUTIIQ). Neurourol Urodyn. 43(4):902-914. https://doi.org/10.1002/nau.25426
The Urology Foundation (2024) The UTI Information Service and Helpline. https://www.theurologyfoundation.org/urology-health/uti-information-service-and-helpline/ (accessed 6 February 2026)
Further reading
Chen YY, Su TH, Lau HH (2021) Estrogen for the prevention of recurrent urinary tract infections in postmenopausal women: a meta-analysis of randomized controlled trials. Int Urogynecol J. 32(1):17-25. https://doi.org/10.1007/s00192-020-04397-z
Harding C, Mossop H, Homer T et al (2022) Alternative to prophylactic antibiotics for the treatment of recurrent urinary tract infections in women: multicentre, open label, randomised, non-inferiority trial. BMJ. 376:e068229. https://doi.org/10.1136/bmj-2021-0068229
National Institute for Health and Care Excellence (2018) Urinary tract infection (catheter associated): antimicrobial prescribing. https://www.nice.org.uk/guidance/ng113 (accessed 13 February 2026)
National Institute for Health and Care Excellence (2023) Urinary tract infections in adults (QS90). https://www.nice.org.uk/guidance/qs90 (accessed 13 February 2026)
National Institute for Health and Care Excellence (2024) Urinary tract infection (recurrent): antimicrobial prescribing (NG112). https://www.nice.org.uk/guidance/ng112 (accessed 13 February 2026)
National Institute for Health and Care Excellence (2025a) Urinary tract infection (lower) - men. https://cks.nice.org.uk/topics/urinary-tract-infection-lower-men/ (accessed 13 February 2026)
National Institute for Health and Care Excellence (2025b) Urinary tract infection (lower) - women. https://cks.nice.org.uk/topics/urinary-tract-infection-lower-women/ (accessed 13 February 2026)
UK Health Security Agency, NHS England (2025) Diagnosis of urinary tract infections: quick reference tools for primary care. https://www.gov.uk/government/publications/urinary-tract-infection-diagnosis/diagnosis-of-urinary-tract-infections-quick-reference-tools-for-primary-care (accessed 6 February 2026)