

Urinary sheaths
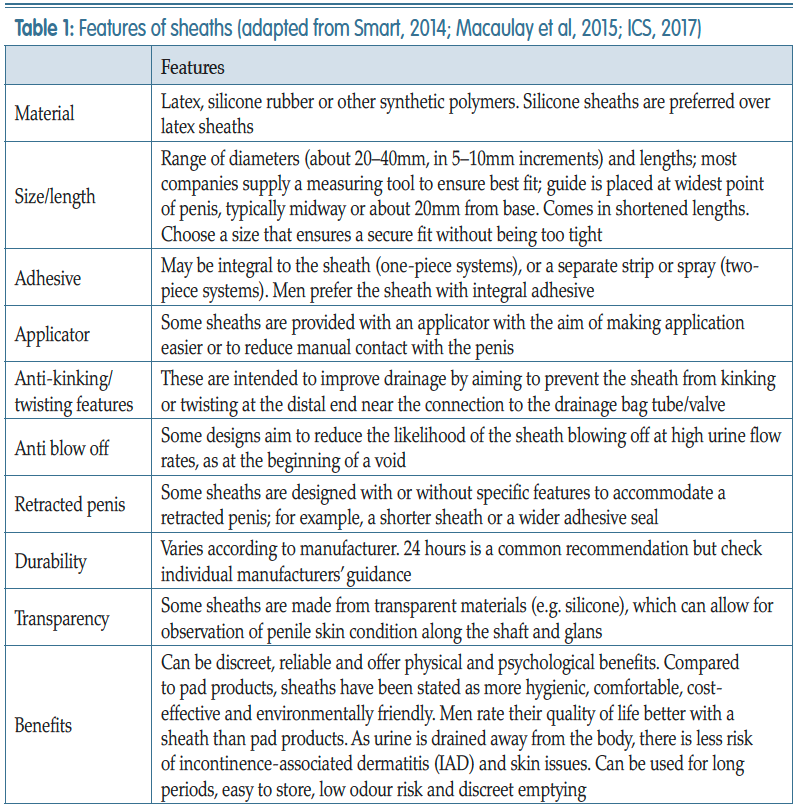
Sheaths, also known as male external catheters (MEC), look in appearance similar to a contraceptive condom (Figure 1). These devices are soft, flexible sleeves designed to fit over the penis and can be attached to a urinary drainage bag or valve. It is vitally important that healthcare professionals are competent in assessing the need for a sheath and have the skill and expertise in applying correctly and passing this knowledge onto the individual. Urinary sheaths have specialised features that need to be considered before being recommended to an individual for use (Table 1).
Figure 1.
Urinary sheaths
To use a sheath, individuals should have good dexterity, some degree of penile length (no retraction), usually have moderate-to-severe urinary incontinence, suffer with urinary urgency/frequency, and find it difficult to get to the toilet in time. Men may use for temporary containment, i.e. travel, shopping or during the night. However there are also some men for whom sheaths would not be advisable or suitable (Table 2).
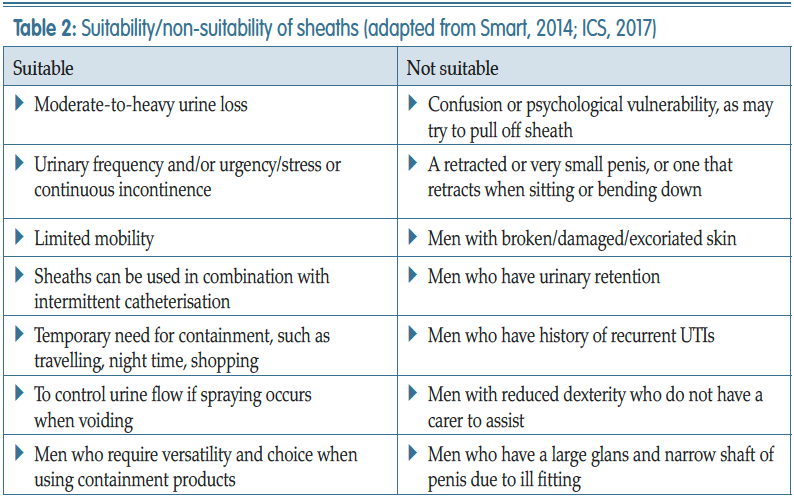

Figure 2
Petal sheaths

Figure 3
PPU with drainage bag.
Figure 4
Penile pouch
.jpg)
Figure 5
Range of penile compression clamps
References
Abrams P, Cardozo L, Fall M, et al (2002) The standardisation of terminology of lower urinary tract function: report from the Standardisation Subcommittee of the International Continence Society. Neurourol Urodyn 21(2): 167–178
Continence Product Advisor (2020) Penile compression devices. Available online: www.continenceproductadvisor.org/products/maledevices/penilecompressiondevices
European Association of Urology Nurses (2008) Good Practice in Health Care: The male external catheter. Available online: https://nurses.uroweb.org/wp-content/uploads/EAUN_MEC_Guidelines_EN_2008_LR.pdf
Haylen BT, de Ridder D, Freeman RM, et al (2010) An international urogynecological association (IUGA)/ international continence society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn 29(1): 4–20
International Continence Society (2017) Incontinence. 6th edn. Editors Abrams P, Cardozo L, Wagg A, Wein A, ICUD ICS Tokyo
Lemmens JMH, Broadbridge J, Macaulay M, Rees RW, Archer M, Drake MJ, Moore KN, Bader DL, Fader M (2019) Tissue response to applied loading using different designs of penile compression clamps. Med Devices (Auckl) 12: 235–243
Lukacz ES, Sampselle C, Gray M, et al (2011) A healthy bladder: a consensus statement. Int J Clin Prac 65(10): 1026–1036
Macaulay M, Broadbridge J, Gage H, Williams P, Birch B, Moore KN, Cottenden A, Fader M (2015) A trial of devices for urinary incontinence after treatment for prostate cancer. BJU Int 116: 432–442
NHS England (2018) Excellence in continence care: Practical guidance for commissioners, and leaders in health and social care. Available online: www.england.nhs.uk/wp-content/uploads/2018/07/excellence-in-continence-care.pdf
National Institute for Health and Care Excellence (2010) Lower urinary tract symptoms in men: management. Clinical Guideline CG97 updated in 2015. Available online: https://www.nice.org.uk/Guidance/CG97
Smart C (2014) Male urinary incontinence and the urinary sheath. Br J Nurs Urol Supp 23(9): S20–S25
Yates A (2017) Urinary continence care for the older people in the acute setting. Br J Nurs 26(9 suppl): S28–S30
Yates A (2019) Basic continence assessment: what community nurses should know. J Community Nurs 33(3): 52–55
Continence Product Advisor (2020) Penile compression devices. Available online: www.continenceproductadvisor.org/products/maledevices/penilecompressiondevices
European Association of Urology Nurses (2008) Good Practice in Health Care: The male external catheter. Available online: https://nurses.uroweb.org/wp-content/uploads/EAUN_MEC_Guidelines_EN_2008_LR.pdf
Haylen BT, de Ridder D, Freeman RM, et al (2010) An international urogynecological association (IUGA)/ international continence society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn 29(1): 4–20
International Continence Society (2017) Incontinence. 6th edn. Editors Abrams P, Cardozo L, Wagg A, Wein A, ICUD ICS Tokyo
Lemmens JMH, Broadbridge J, Macaulay M, Rees RW, Archer M, Drake MJ, Moore KN, Bader DL, Fader M (2019) Tissue response to applied loading using different designs of penile compression clamps. Med Devices (Auckl) 12: 235–243
Lukacz ES, Sampselle C, Gray M, et al (2011) A healthy bladder: a consensus statement. Int J Clin Prac 65(10): 1026–1036
Macaulay M, Broadbridge J, Gage H, Williams P, Birch B, Moore KN, Cottenden A, Fader M (2015) A trial of devices for urinary incontinence after treatment for prostate cancer. BJU Int 116: 432–442
NHS England (2018) Excellence in continence care: Practical guidance for commissioners, and leaders in health and social care. Available online: www.england.nhs.uk/wp-content/uploads/2018/07/excellence-in-continence-care.pdf
National Institute for Health and Care Excellence (2010) Lower urinary tract symptoms in men: management. Clinical Guideline CG97 updated in 2015. Available online: https://www.nice.org.uk/Guidance/CG97
Smart C (2014) Male urinary incontinence and the urinary sheath. Br J Nurs Urol Supp 23(9): S20–S25
Yates A (2017) Urinary continence care for the older people in the acute setting. Br J Nurs 26(9 suppl): S28–S30
Yates A (2019) Basic continence assessment: what community nurses should know. J Community Nurs 33(3): 52–55