


Figure 1. Uresta intravaginal device.

Figure 2. Diveen and applicator intravaginal device.
Figure 3. Contiform intravaginal device.
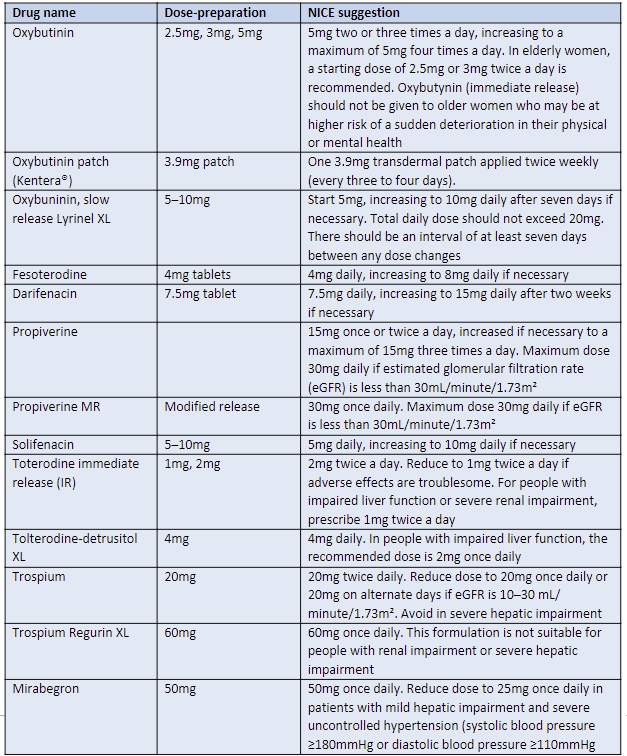
Table 4. Medications available for OAB. (Adapted from NICE, 2019)
Changing the pessary
Following removal of the vaginal pessary, the condition of vaginal tissues should be checked using a speculum. Atrophic tissues should be noted and a topical vaginal oestrogen in the form of a cream or pessary tablet should be considered (Bulchandani et al, 2014). The pessary device should be left out if there is evidence of bleeding and/ or ulceration, which will allow for the tissues to heal (Stewart, 2019). If the woman is post-menopausal, has a womb and notices vaginal bleeding when she has a pessary, she should be referred to secondary care on the two-week wait pathway for assessment of endometrial thickness and screening for possible endometrial cancer. An endometrial biopsy should be considered to exclude coexisting endometrial cancer (Vanichtantikul et al, 2017).
The most common cause for vaginal bleeding in women who have a vaginal pessary is atrophic vaginitis (Figure 4) — this is when the tissues in the vagina lack oestrogen and become dry and thin. This may cause bleeding (Domoney, 2014), as the pessary rubs inside the vagina as the patient moves around.
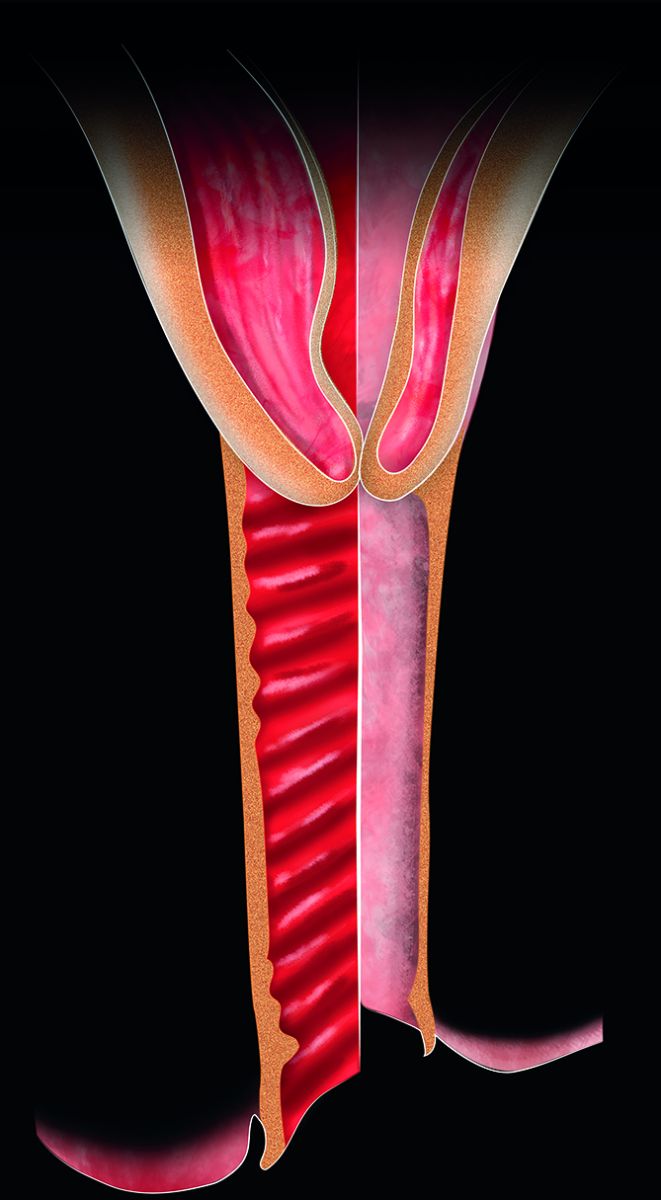
Figure 4. Atrophic vaginal tissues.
References
Bo K, Frawley H, Haylen B, Abarmov Y, Almeida F, Bergmans B, et al (2017) International Urogynaecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for the conservative and non-pharmacological management of female pelvic floor dysfunction: Terminology for Female Pelvic Floor Dysfunction. Int Urogynaecology J 28(2): 191–213
Brucker B, Lee, R, Newman K (2020) Optimizing nonsurgical treatments of overactive bladder in the United States. Urology 145: 52–9
Bulchandani S, Tooz-Hobson P, Verghese T, et al (2014) Does vaginal oestrogen treatment with support pessaries in vaginal prolapse reduce complications? Post Reprod Health 21(4): 141–5
Chung S, Kim W (2018) Various approaches and treatments for pelvic organ prolapse in women. J Menopausal Med 24: 155–62
Dhaliwal P, Wagg A (2016) Overactive bladder: strategies to ensure treatment compliance and adherence. Clin Interv Aging 11: 755–60
DeMaagd G, Davenport T (2012) Management of urinary incontinence. PT 37(6): 345-621
Dicker D, Alfadda A, Coutinho W, et al (2021) Patient motivation to lose weight: importance of healthcare professional support, goals and self-efficacy. Eur J Internal Med 91: 10–16
Domoney C (2014) Treatment of vaginal atrophy. Women’s Health 10(2): 191–200
Dwyer L, Stewart E, Rajai A (2021) A service evaluation to determine where and who delivers pessary care in the UK. Int J Urogynaecol 32(4): 1001–6
Faiena I, Patel N, Parihar JS, et al (2015) Conservative management of urinary incontinence in women. Rev Urol 17(3): 129–39
Fontaine C, Papworth E, Pascoe J (2021) Update on the management of overactive bladder. Ther Adv Urol 13: 17562872211
International Continence Society (2018) Stress Urinary Incontinence. Available online: www.ics.org/committees/standardisation/terminologydiscussions/sui
Jones K, Harmanli O (2010) Pessary use in pelvic organ prolapse and urinary incontinence. Rev Obstet Gynecol 3(1): 3–9
Mazur-Bialy A, Kolomanska-Bogucka D, Nowakowski C, Tim S (2020) Urinary incontinence in women: modern methods of physiotherapy as a support for surgical treatment or independent therapy. J Clin Med 9(4): 1211
NHS (2022) The NHS Digital Weight Management Programme. Available online: www.england.nhs.uk/digital-weightmanagement/
National Institute for Health and Care Excellence (2013) Urinary incontinence in women: management. CG171. NICE, London. Available online: www.nice.org.uk/guidance/cg171
National Institute for Health and Care Excellence (2017) Urinary Incontinence in Women: management clinical guideline. NICE, London. Available online: www.nice.org.uk/guidance/cg171
National Institute for Health and Care Excellence (2019a) Incontinence: urinary, in women; Antimuscarinics. NICE, London. Available online: https://cks.nice.org.uk/topics/incontinence-urinary-in-women/prescribing-information/antimuscarinics/
National Institute for Health and Care Excellence (2019b) Urinary incontinence and pelvic organ prolapse in women: management. NICE guideline [NG123]. NICE, London. Available online: www.nice.org.uk/guidance/ng123
National Institure for Health and Care Excellence (2021) Pelvic floor dysfunction: prevention and non-surgical management. NICE guideline [NG210]. NICE, London. Available online: www.nice.org.uk/guidance/ng210
National Institute for Health and Care Excellence/BNF (2022) Antimuscarinics (systemic). Available online: https://bnf.nice.org.uk/drug-class/antimuscarinicssystemic.html
National Institute for Health and Care Excellence/BNF (2022) Duloxetine. Available online: https://bnf.nice.org.uk/drug/duloxetine.html
Noble N (2018) Female urinary incontinence: pharmacological treatments. Nurse Prescribing 16(3): 116–20
Okeahialam N, Dworzynski K, Jacklin P, et al (2022) Prevention and non-surgical management of pelvic floor dysfunction: summary of NICE Guidelines. BMJ 376: n3049
Ostle Z (2016) Assessment, diagnosis and treatment of urinary incontinence in women. Br J Nurs 25(2): 84–91
Pomian A, Lisik W, Kosieradzki M (2016) Obesity and pelvic floor disorders: a review of the literature. Med Sci Monit 22: 1880–6
Rantell A (2015) Understanding urinary incontinence in women. Practice Nursing 26(6): 275–81
Sudol N, Adams-Piper E, Perry R, Lane F, Chen K (2019) In search of mobile applications for patients with pelvic floor disorders. Female Pelvic Med Reconstr 25(3): 252–6
Stewart E (2019) Urogynaecology. In: Holloway D, ed. Nursing management of women’s health: A guide for nurse specialists and practitioners. Springer: 215–34
United Kingdom Continence Society. UK Clinical Guideline: for best practice in the use of vaginal pessaries for pelvic organ prolapse (launched March 20221). Available online: www.ukcs.uk.net/UK-PessaryGuideline-2021
Vanichtantikul A, Tharavichitkul E, Chitapanarux I, Chinthakanan O (2017) Treatment of endometrial cancer in association with pelvic organ prolapse. Case Rep Obstet Gynecol 2017: 1640614
Zeiger B, Da Silva Carramao S, Del Roy C, et al (2021) Vaginal pessary in advanced pelvic organ prolapse: impact on quality of life. Int Urogynaecol J Nov 6: 1–8
Brucker B, Lee, R, Newman K (2020) Optimizing nonsurgical treatments of overactive bladder in the United States. Urology 145: 52–9
Bulchandani S, Tooz-Hobson P, Verghese T, et al (2014) Does vaginal oestrogen treatment with support pessaries in vaginal prolapse reduce complications? Post Reprod Health 21(4): 141–5
Chung S, Kim W (2018) Various approaches and treatments for pelvic organ prolapse in women. J Menopausal Med 24: 155–62
Dhaliwal P, Wagg A (2016) Overactive bladder: strategies to ensure treatment compliance and adherence. Clin Interv Aging 11: 755–60
DeMaagd G, Davenport T (2012) Management of urinary incontinence. PT 37(6): 345-621
Dicker D, Alfadda A, Coutinho W, et al (2021) Patient motivation to lose weight: importance of healthcare professional support, goals and self-efficacy. Eur J Internal Med 91: 10–16
Domoney C (2014) Treatment of vaginal atrophy. Women’s Health 10(2): 191–200
Dwyer L, Stewart E, Rajai A (2021) A service evaluation to determine where and who delivers pessary care in the UK. Int J Urogynaecol 32(4): 1001–6
Faiena I, Patel N, Parihar JS, et al (2015) Conservative management of urinary incontinence in women. Rev Urol 17(3): 129–39
Fontaine C, Papworth E, Pascoe J (2021) Update on the management of overactive bladder. Ther Adv Urol 13: 17562872211
International Continence Society (2018) Stress Urinary Incontinence. Available online: www.ics.org/committees/standardisation/terminologydiscussions/sui
Jones K, Harmanli O (2010) Pessary use in pelvic organ prolapse and urinary incontinence. Rev Obstet Gynecol 3(1): 3–9
Mazur-Bialy A, Kolomanska-Bogucka D, Nowakowski C, Tim S (2020) Urinary incontinence in women: modern methods of physiotherapy as a support for surgical treatment or independent therapy. J Clin Med 9(4): 1211
NHS (2022) The NHS Digital Weight Management Programme. Available online: www.england.nhs.uk/digital-weightmanagement/
National Institute for Health and Care Excellence (2013) Urinary incontinence in women: management. CG171. NICE, London. Available online: www.nice.org.uk/guidance/cg171
National Institute for Health and Care Excellence (2017) Urinary Incontinence in Women: management clinical guideline. NICE, London. Available online: www.nice.org.uk/guidance/cg171
National Institute for Health and Care Excellence (2019a) Incontinence: urinary, in women; Antimuscarinics. NICE, London. Available online: https://cks.nice.org.uk/topics/incontinence-urinary-in-women/prescribing-information/antimuscarinics/
National Institute for Health and Care Excellence (2019b) Urinary incontinence and pelvic organ prolapse in women: management. NICE guideline [NG123]. NICE, London. Available online: www.nice.org.uk/guidance/ng123
National Institure for Health and Care Excellence (2021) Pelvic floor dysfunction: prevention and non-surgical management. NICE guideline [NG210]. NICE, London. Available online: www.nice.org.uk/guidance/ng210
National Institute for Health and Care Excellence/BNF (2022) Antimuscarinics (systemic). Available online: https://bnf.nice.org.uk/drug-class/antimuscarinicssystemic.html
National Institute for Health and Care Excellence/BNF (2022) Duloxetine. Available online: https://bnf.nice.org.uk/drug/duloxetine.html
Noble N (2018) Female urinary incontinence: pharmacological treatments. Nurse Prescribing 16(3): 116–20
Okeahialam N, Dworzynski K, Jacklin P, et al (2022) Prevention and non-surgical management of pelvic floor dysfunction: summary of NICE Guidelines. BMJ 376: n3049
Ostle Z (2016) Assessment, diagnosis and treatment of urinary incontinence in women. Br J Nurs 25(2): 84–91
Pomian A, Lisik W, Kosieradzki M (2016) Obesity and pelvic floor disorders: a review of the literature. Med Sci Monit 22: 1880–6
Rantell A (2015) Understanding urinary incontinence in women. Practice Nursing 26(6): 275–81
Sudol N, Adams-Piper E, Perry R, Lane F, Chen K (2019) In search of mobile applications for patients with pelvic floor disorders. Female Pelvic Med Reconstr 25(3): 252–6
Stewart E (2019) Urogynaecology. In: Holloway D, ed. Nursing management of women’s health: A guide for nurse specialists and practitioners. Springer: 215–34
United Kingdom Continence Society. UK Clinical Guideline: for best practice in the use of vaginal pessaries for pelvic organ prolapse (launched March 20221). Available online: www.ukcs.uk.net/UK-PessaryGuideline-2021
Vanichtantikul A, Tharavichitkul E, Chitapanarux I, Chinthakanan O (2017) Treatment of endometrial cancer in association with pelvic organ prolapse. Case Rep Obstet Gynecol 2017: 1640614
Zeiger B, Da Silva Carramao S, Del Roy C, et al (2021) Vaginal pessary in advanced pelvic organ prolapse: impact on quality of life. Int Urogynaecol J Nov 6: 1–8
This piece was first published in the Journal of General Practice Nursing. To cite this article use: Stewart E (2022) Treatments for female urinary incontinence and pelvic organ prolapse. J Gen Pract Nurs 8(1): 47-53