

There remains a stigma attached to our natural daily ablutions, which means that common bowel dysfunctions, such as constipation or lack of control, are kept hidden. People are embarrassed to admit they have problems. They feel ashamed due to a perceived loss of dignity, so they keep quiet and, by doing so, they shield the fact that bowel conditions are incredibly common. In fact, according to a Coloplast report on the cost of constipation (2015), one in seven people experiences a problem with bowel incontinence. Although that means a large number of people require some medical treatment, many delay seeking help for manageable conditions, or they assume that support is not available (NHS Choices, 2012).
Unfortunately, bowel dysfunction is often misunderstood by healthcare professionals and when patients do decide to seek medical help, it is not always up to standard. You would expect the NHS to provide reassurance, empathy and high quality clinical care for these people who may be feeling vulnerable and ashamed and whose bowel issues may be affecting their quality of life. However, a report titled ‘Raising Expectations for People with Bladder and Bowel Problems’ (2015) found that patients with these issues were not treated with dignity and respect. Based on insights gathered through a small qualitative workshop and supported by evidence collected through national clinical audits (Royal College of Physicians [RCP], 2010), the report highlighted that patients did not feel listened to or taken seriously when they first sought help from their doctor. They also lacked confidence that clinicians understood their symptoms or knew how to treat them, and they felt that they were not offered adequate information about their condition or treatment options. Additionally, they did not feel involved in decisions made about their treatment and care, or have access to the highquality interventions that have been recommended by the National Institute for Health and Care Excellence (NICE).
 It is sobering reading, as bladder and bowel dysfunctions lack the same ‘status’ as more recognised chronic conditions, even though the effect of moderate continence issues on quality of life is similar to living with diabetes, hypertension or cancer (Robertson et al, 2007). This means that patients often fail to get even the most basic aspects of care correctly. However, given that poor continence care compromises fundamental NHS rights to dignity and respect, it is essential that addressing these shortcomings must now become a priority. Of the 33 cases presented as oral evidence to the Francis Inquiry into care provided by Mid Staffordshire NHS Foundation Trust, 22 included ‘significant concerns’ about continence care, which led to ‘considerable suffering, distress and embarrassment’ to patients (Francis, 2010).
It is sobering reading, as bladder and bowel dysfunctions lack the same ‘status’ as more recognised chronic conditions, even though the effect of moderate continence issues on quality of life is similar to living with diabetes, hypertension or cancer (Robertson et al, 2007). This means that patients often fail to get even the most basic aspects of care correctly. However, given that poor continence care compromises fundamental NHS rights to dignity and respect, it is essential that addressing these shortcomings must now become a priority. Of the 33 cases presented as oral evidence to the Francis Inquiry into care provided by Mid Staffordshire NHS Foundation Trust, 22 included ‘significant concerns’ about continence care, which led to ‘considerable suffering, distress and embarrassment’ to patients (Francis, 2010).
Age is a major risk factor for bladder and bowel dysfunction and as the population ages, demand for treatment and care will continue to grow (Department of Health [DH, 2000).
Delayed, inadequate care is costly to the patient healthwise, and it is expensive for the NHS. Unmanaged symptoms can lead to avoidable issues such as urinary tract infection (UTI), pressure ulcers and falls, which result in an increase in service use and prescriptions costs (Health and Social Care Partnership, 2011; Expert Group on Lower Urinary Tract Symptoms, 2012). Urinary incontinence is associated with a number of comorbidities such as arthritis, asthma, chronic anxiety, depression, diabetes, neurological conditions, sleep disorders (Coyne et al, 2009), dementia, heart and kidney diseases (European Association of Urology, 2011), and if outcomes for patients with those issues are to be improved, incontinence cannot be overlooked.
Bladder and bowel issues have to be taken seriously and for that to happen healthcare professionals need to be more open about them. The ‘Raising Expectations for People with Bladder and Bowel Problems’ (2015) report urges the government, NHS leaders, commissioners, providers, healthcare professionals and patients to start talking about common problems of incontinence, and other issues, and to consider what steps they can take to raise expectations for people with these dysfunctions. The purpose of this article is to see what it is like to experience and cope with bowel problems, specifically the common problem of constipation. It also establishes a number of imperatives for the development of NHS practice and policy to improve patient experiences and outcomes through more proactive and costeffective models of care.
‘... bladder and bowel dysfunctions lack the same “status” as more recognised chronic conditions, even though the effect of moderate continence issues on quality of life is similar... .’
Unfortunately, bowel dysfunction is often misunderstood by healthcare professionals and when patients do decide to seek medical help, it is not always up to standard. You would expect the NHS to provide reassurance, empathy and high quality clinical care for these people who may be feeling vulnerable and ashamed and whose bowel issues may be affecting their quality of life. However, a report titled ‘Raising Expectations for People with Bladder and Bowel Problems’ (2015) found that patients with these issues were not treated with dignity and respect. Based on insights gathered through a small qualitative workshop and supported by evidence collected through national clinical audits (Royal College of Physicians [RCP], 2010), the report highlighted that patients did not feel listened to or taken seriously when they first sought help from their doctor. They also lacked confidence that clinicians understood their symptoms or knew how to treat them, and they felt that they were not offered adequate information about their condition or treatment options. Additionally, they did not feel involved in decisions made about their treatment and care, or have access to the highquality interventions that have been recommended by the National Institute for Health and Care Excellence (NICE).
It is sobering reading, as bladder and bowel dysfunctions lack the same ‘status’ as more recognised chronic conditions, even though the effect of moderate continence issues on quality of life is similar to living with diabetes, hypertension or cancer (Robertson et al, 2007). This means that patients often fail to get even the most basic aspects of care correctly. However, given that poor continence care compromises fundamental NHS rights to dignity and respect, it is essential that addressing these shortcomings must now become a priority. Of the 33 cases presented as oral evidence to the Francis Inquiry into care provided by Mid Staffordshire NHS Foundation Trust, 22 included ‘significant concerns’ about continence care, which led to ‘considerable suffering, distress and embarrassment’ to patients (Francis, 2010).Age is a major risk factor for bladder and bowel dysfunction and as the population ages, demand for treatment and care will continue to grow (Department of Health [DH, 2000).
Delayed, inadequate care is costly to the patient healthwise, and it is expensive for the NHS. Unmanaged symptoms can lead to avoidable issues such as urinary tract infection (UTI), pressure ulcers and falls, which result in an increase in service use and prescriptions costs (Health and Social Care Partnership, 2011; Expert Group on Lower Urinary Tract Symptoms, 2012). Urinary incontinence is associated with a number of comorbidities such as arthritis, asthma, chronic anxiety, depression, diabetes, neurological conditions, sleep disorders (Coyne et al, 2009), dementia, heart and kidney diseases (European Association of Urology, 2011), and if outcomes for patients with those issues are to be improved, incontinence cannot be overlooked.
Bladder and bowel issues have to be taken seriously and for that to happen healthcare professionals need to be more open about them. The ‘Raising Expectations for People with Bladder and Bowel Problems’ (2015) report urges the government, NHS leaders, commissioners, providers, healthcare professionals and patients to start talking about common problems of incontinence, and other issues, and to consider what steps they can take to raise expectations for people with these dysfunctions. The purpose of this article is to see what it is like to experience and cope with bowel problems, specifically the common problem of constipation. It also establishes a number of imperatives for the development of NHS practice and policy to improve patient experiences and outcomes through more proactive and costeffective models of care.
TYPES OF CONSTIPATION
 Constipation comes in two forms: slow colonic transit or difficulties with evacuation, and it is possible for patients to have both. Those suffering from slow colonic transit tend to complain that they rarely feel the urge to go to the toilet and some cannot go at all unless they take laxatives. According to the Coloplast (2015) report on the cost of constipation, sufferers can be divided into two groups: ‘functional’ and ‘neurogenic’. The majority of people fall into the ‘functional’ category.
Constipation comes in two forms: slow colonic transit or difficulties with evacuation, and it is possible for patients to have both. Those suffering from slow colonic transit tend to complain that they rarely feel the urge to go to the toilet and some cannot go at all unless they take laxatives. According to the Coloplast (2015) report on the cost of constipation, sufferers can be divided into two groups: ‘functional’ and ‘neurogenic’. The majority of people fall into the ‘functional’ category.Functional constipation is diagnosed when a person is experiencing symptoms, but there are no underlying known bowel problems and all of the organs in the body are working (RCN, 2015). Most of these people would not consider visiting their GP due to embarrassment or fear that it may be the result of a more serious underlying condition. Although this is rarely the case, it is best to rule these worries out by speaking to a GP or healthcare provider.
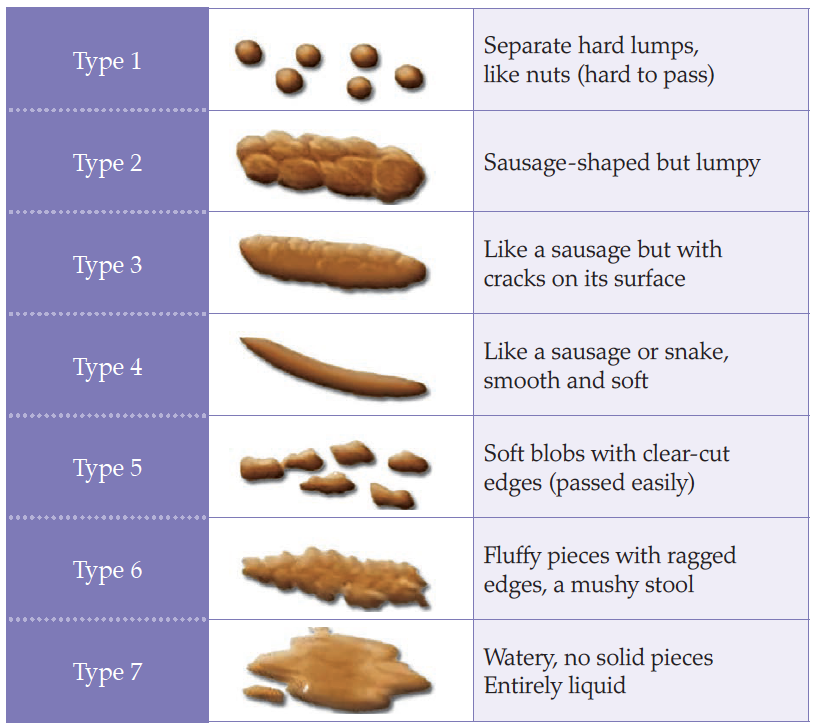
Figure 1.
Bristol stool chart.
 Obstructive defecation syndrome, or rectal outlet delay, is defined as a sensation of anal blockage on more than one in four occasions, prolonged elimination taking more than 10 minutes to complete evacuation, or the need to use fingers on any occasion (Harari, 2004). Faecal impaction, or loading, is when the rectum and often the lower colon is full of hard or soft stool and the patient is unable to evacuate the bowel unaided (Norton, 2006). This can lead to impaction with overflow ‘spurious diarrhoea’, which is common in the frail elderly population (Harari, 2004) and may be misdiagnosed as diarrhoea and therefore treated incorrectly (Norton, 2006).
Obstructive defecation syndrome, or rectal outlet delay, is defined as a sensation of anal blockage on more than one in four occasions, prolonged elimination taking more than 10 minutes to complete evacuation, or the need to use fingers on any occasion (Harari, 2004). Faecal impaction, or loading, is when the rectum and often the lower colon is full of hard or soft stool and the patient is unable to evacuate the bowel unaided (Norton, 2006). This can lead to impaction with overflow ‘spurious diarrhoea’, which is common in the frail elderly population (Harari, 2004) and may be misdiagnosed as diarrhoea and therefore treated incorrectly (Norton, 2006).Constipation, especially when chronic, can have damaging effects on the colon. The colon is constantly extracting water from its contents to transform liquid wastes into solids. If elimination is not regular and complete, the wastes will dry and become cemented to the walls of the colon. Constipation has been shown to increase the risk of colon cancer (American College of Gastroenterology 2012), and has been implicated in diverticulitis and appendicitis. It is essential that it is treated as a serious condition.
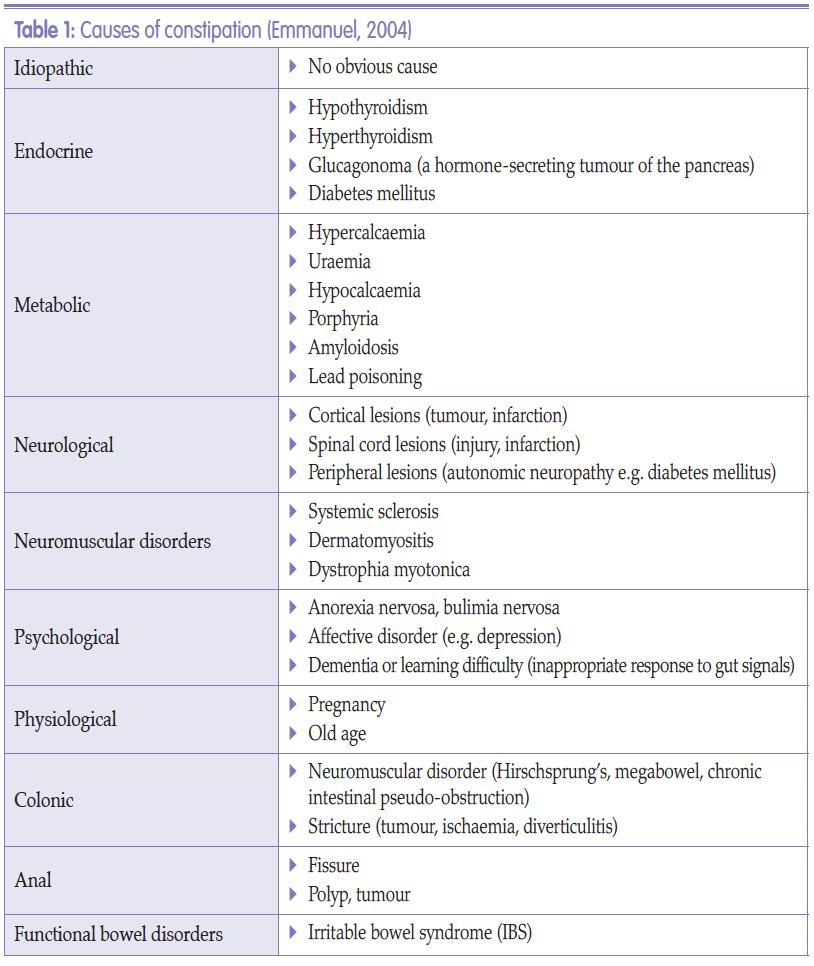
There are many causes of constipation as illustrated in Table 1.
References
American College of Gastroenterology (2012) Chronic constipation linked to increased risk of colorectal cancer. ScienceDaily, 22 October. Available online: www.sciencedaily.com/releases/2012/10/121022081228.htm
Bladder and Bowel Community (2017) Toilet Positions. Available online: www.bladderandbowel.org/help-information/resources/toilet-positions
Coloplast (2015) The Cost of Constipation Report. Available online: www.coloplast. co.uk/Global/UK/Continence/Cost_of_ Constipation_Report_FINAL.pdf
Commissioning for incontinence, lower urinary tract and bowel symptoms — an audit (2012). Available online: http://ici-rs.net/PDFs/Commissioningforincontinencel owerurinarytractandbowelsymptomsanaudit_ 2.pdf
Coyne KS, Kaplan SA, Chapple CR, et al (2009) Risk factors and comorbid conditions associated with lower urinary tract symptoms: EpiLUTS. BJU Int 103(3): 24–32
Department of Health (2000) Good practice in continence services. DH, London. Available online: www.nhs.uk/chq/Documents/2015%20uploads/DH%20-%20Good%20practice%20in%20 continence%20services.pdf
Emmanuel A (2004) Constipation. In: Norton C, Chelvanayagam S, eds. Bowel Continence Nursing. Beaconsfield Publishers Ltd. Chap 21: 238–50
European Association of Urology (2011) History examination in neurogenic lower urinary tract dysfunction. Available online: www.uroweb.org/gls/pdf/17_Neurogenic%20LUTS.pdf
Francis R (2010) Robert Francis Inquiry report into Mid-Staffordshire NHS Foundation Trust. Available online: http://webarchive. nationalarchives.gov.uk/20130104234315/ http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_113018
Frattini JC, Nogueras JJ (2008) Slow transit constipation: a review of a colonic functional disorder. Clin Colon Rectal Surg 21(2): 146–52
Harari D (2004) Bowel care in old age. In: Norton C, Chelvanayagam S, eds. Bowel Continence Nursing. Beaconsfield Publishers Ltd. Chap 13: 132–50 Health and Social Care Partnership South East (2011) Prevention and early intervention continence services, July Longstreth G, Thompson G, Chey W, Houghton L, Mearin F and Spiller R (2006) Functional bowel disorder, Gastroenterol 130: 1480–91
NHS Choices (2012) The taboo of incontinence. Available online: www.nhs.uk/Livewell/incontinence/Pages/Breakingthetaboo.aspx
Norton C (2001) Nursing for continence. Beaconsfield Publishers Ltd
Norton C (2006) Constipation in older patients: effects on quality of life. Br J Nurs 15(4): 188–92
Norton C , Chelvanayagam S, eds (2004) Bowel Continence Nursing. Beaconsfield Publishers Ltd, Beaconsfield
Raising Expectations for People with Bladder and Bowel Problems (2015) developed by the Bladder and Bowel Foundation (B&BF), Cystitis and Overactive Bladder Foundation (COB), Association for Continence Advice and expert group on lower urinary tract symptoms (LUTS). London: Astellas Pharma Ltd
Rex J (2013) Treatments for Bowel Dysfunction available on YouTube
Robertson C, Link CL, Onel E, et al (2007) The impact of lower urinary tract symptoms and comorbidities on quality of life: the BACH and UREPIK studies. BJU Int 99(2): 347–54
Royal College of Nursing (2008) Bowel care, including digital rectal examination and manual removal of faeces: RCN guidance for nurses. RCN, London
Royal College of Physicians (2010) National audit of continence care: combined organisational and clinical report. RCP, London. Available online: www.rcplondon.ac.uk/sies/default/files/full-organisational-and-clinical-reportnacc- 2010.pdf
Bladder and Bowel Community (2017) Toilet Positions. Available online: www.bladderandbowel.org/help-information/resources/toilet-positions
Coloplast (2015) The Cost of Constipation Report. Available online: www.coloplast. co.uk/Global/UK/Continence/Cost_of_ Constipation_Report_FINAL.pdf
Commissioning for incontinence, lower urinary tract and bowel symptoms — an audit (2012). Available online: http://ici-rs.net/PDFs/Commissioningforincontinencel owerurinarytractandbowelsymptomsanaudit_ 2.pdf
Coyne KS, Kaplan SA, Chapple CR, et al (2009) Risk factors and comorbid conditions associated with lower urinary tract symptoms: EpiLUTS. BJU Int 103(3): 24–32
Department of Health (2000) Good practice in continence services. DH, London. Available online: www.nhs.uk/chq/Documents/2015%20uploads/DH%20-%20Good%20practice%20in%20 continence%20services.pdf
Emmanuel A (2004) Constipation. In: Norton C, Chelvanayagam S, eds. Bowel Continence Nursing. Beaconsfield Publishers Ltd. Chap 21: 238–50
European Association of Urology (2011) History examination in neurogenic lower urinary tract dysfunction. Available online: www.uroweb.org/gls/pdf/17_Neurogenic%20LUTS.pdf
Francis R (2010) Robert Francis Inquiry report into Mid-Staffordshire NHS Foundation Trust. Available online: http://webarchive. nationalarchives.gov.uk/20130104234315/ http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_113018
Frattini JC, Nogueras JJ (2008) Slow transit constipation: a review of a colonic functional disorder. Clin Colon Rectal Surg 21(2): 146–52
Harari D (2004) Bowel care in old age. In: Norton C, Chelvanayagam S, eds. Bowel Continence Nursing. Beaconsfield Publishers Ltd. Chap 13: 132–50 Health and Social Care Partnership South East (2011) Prevention and early intervention continence services, July Longstreth G, Thompson G, Chey W, Houghton L, Mearin F and Spiller R (2006) Functional bowel disorder, Gastroenterol 130: 1480–91
NHS Choices (2012) The taboo of incontinence. Available online: www.nhs.uk/Livewell/incontinence/Pages/Breakingthetaboo.aspx
Norton C (2001) Nursing for continence. Beaconsfield Publishers Ltd
Norton C (2006) Constipation in older patients: effects on quality of life. Br J Nurs 15(4): 188–92
Norton C , Chelvanayagam S, eds (2004) Bowel Continence Nursing. Beaconsfield Publishers Ltd, Beaconsfield
Raising Expectations for People with Bladder and Bowel Problems (2015) developed by the Bladder and Bowel Foundation (B&BF), Cystitis and Overactive Bladder Foundation (COB), Association for Continence Advice and expert group on lower urinary tract symptoms (LUTS). London: Astellas Pharma Ltd
Rex J (2013) Treatments for Bowel Dysfunction available on YouTube
Robertson C, Link CL, Onel E, et al (2007) The impact of lower urinary tract symptoms and comorbidities on quality of life: the BACH and UREPIK studies. BJU Int 99(2): 347–54
Royal College of Nursing (2008) Bowel care, including digital rectal examination and manual removal of faeces: RCN guidance for nurses. RCN, London
Royal College of Physicians (2010) National audit of continence care: combined organisational and clinical report. RCP, London. Available online: www.rcplondon.ac.uk/sies/default/files/full-organisational-and-clinical-reportnacc- 2010.pdf