

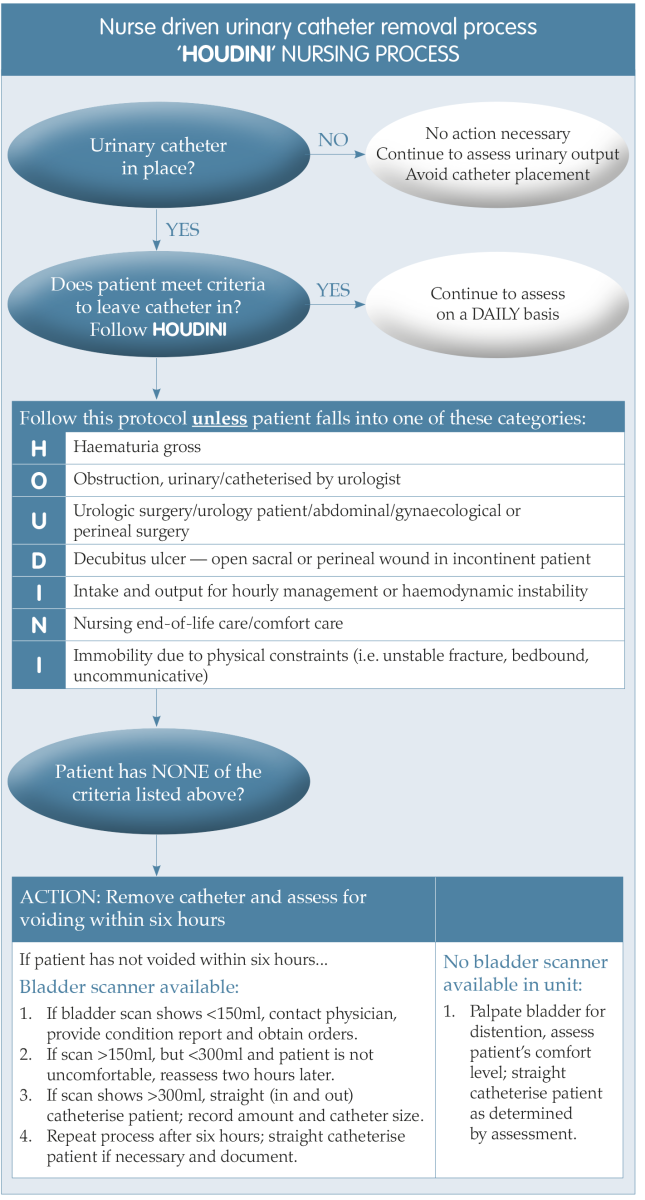
Figure 1. A nurse driven process for timely removal of urinary catheters (Yatim et al, 2016).
.png)
Table 1. Root cause analysis process (adapted from National Patient Safety Agency, 2004)
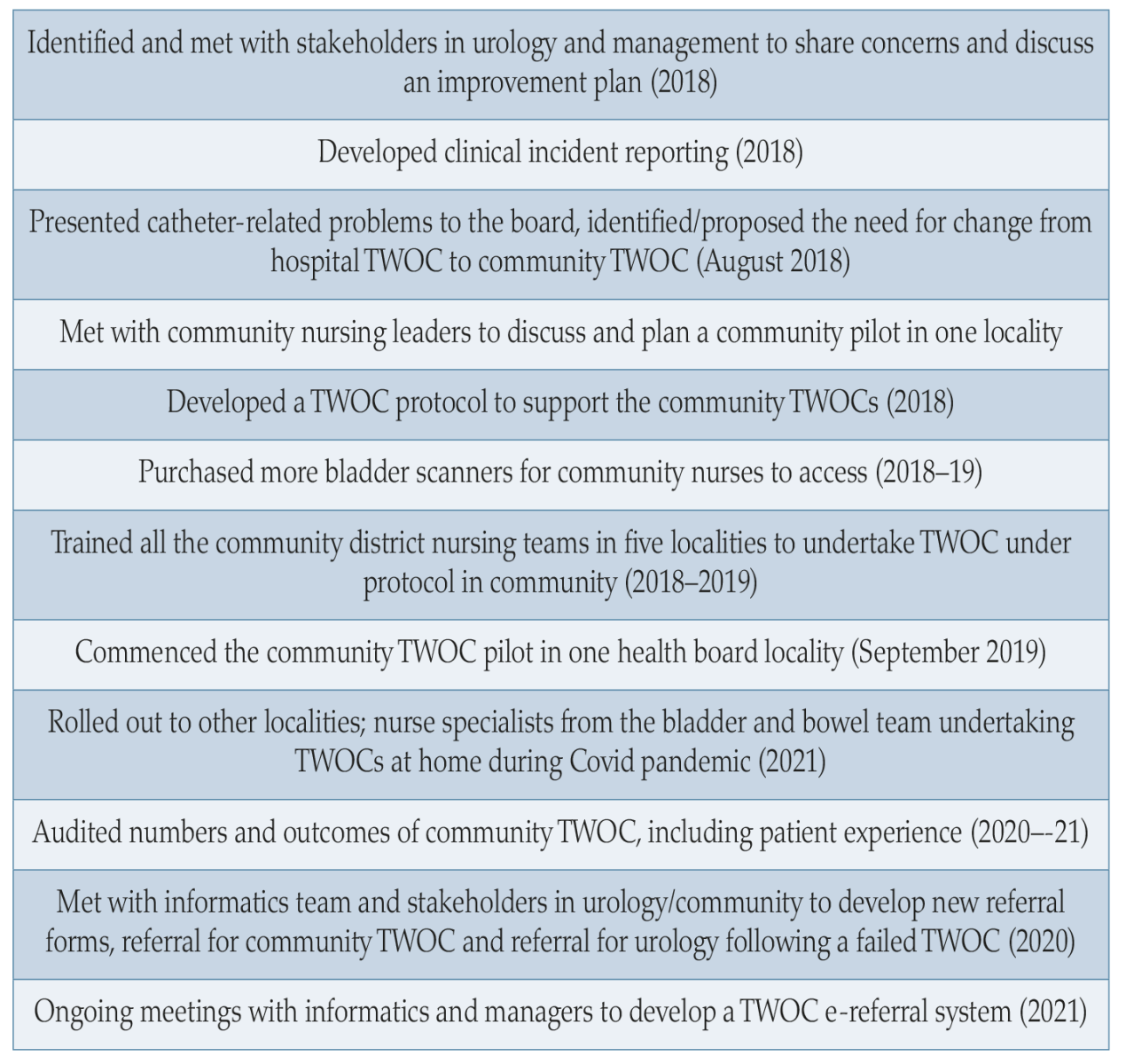
Figure 2. Service development stages and timescales.
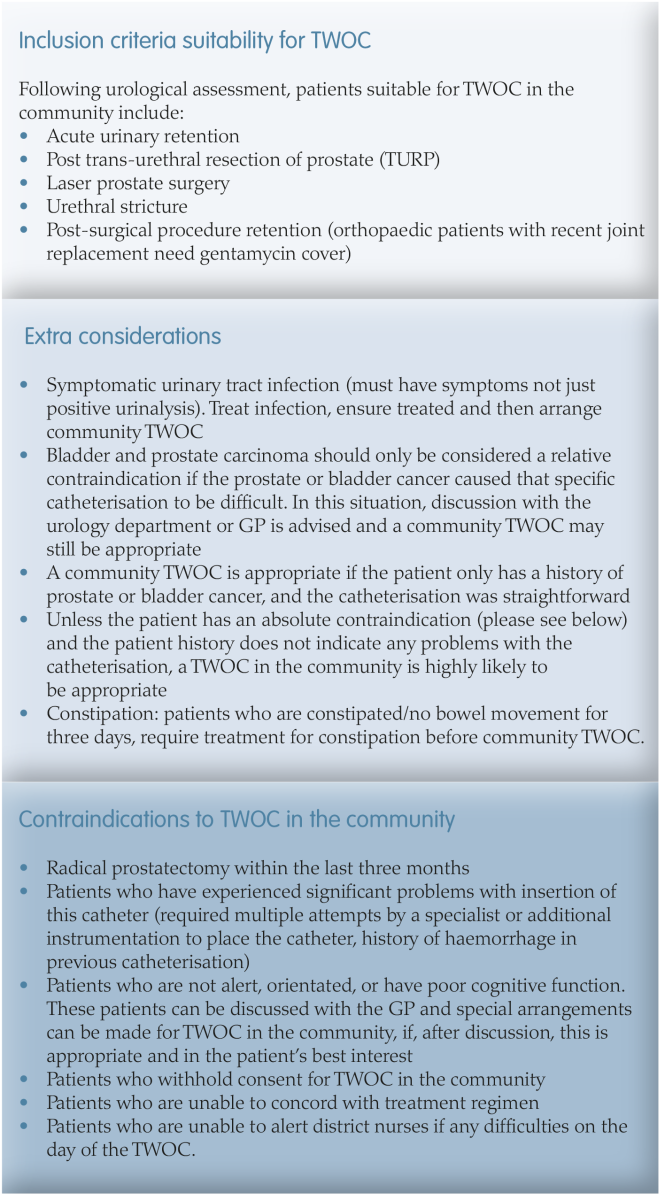
Figure 3. Inclusion and exclusion criteria.
COMMUNITY TWOC PILOT AND THE ROLL OUT
The pilot started in one locality within the health board and subsequently rolled out across the other four once training in TWOC had been delivered to the community nurses. It is recommended that trained and experienced healthcare professionals who can monitor and determine the success of the procedure are available to undertake TWOCs guided by a clear followup protocol (Gilbert, 2006 cited in Holroyd, 2020).
Audit results
The pilot was audited to monitor the number of TWOCs undertaken and clinical outcomes. The project incorporated user involvement and participation, which is important in understanding patient experiences and developing services. Audit data was collected and analysed between April 2020 and March 2021:
- 276 patients referred to bladder and bowel service for a TWOC:
○ Average age 75.5 years
○ Average length of wait for TWOC — five weeks - 62% (182) patients had a community TWOC
- Reasons for not undergoing community TWOC:
○ RIP
○ Declined
○ Previously TWOCed by urology/district nurse
○ Inappropriate referral.
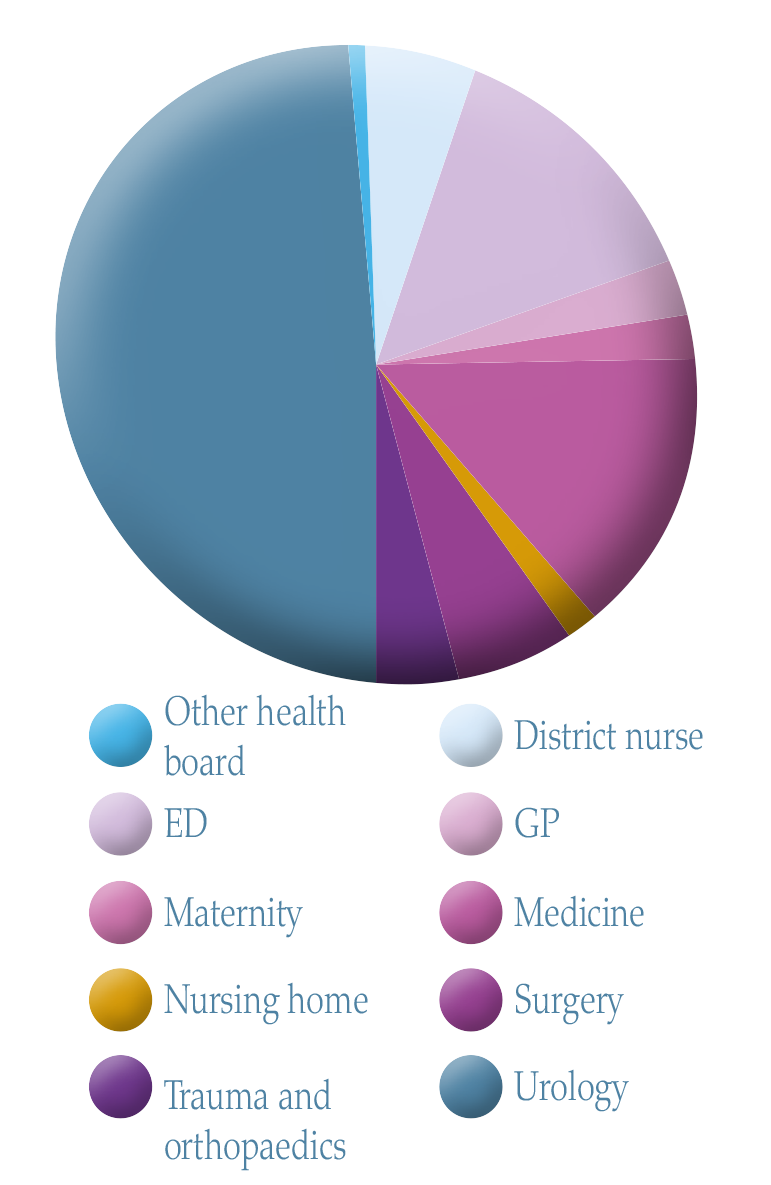
Figure 5. Referral source.
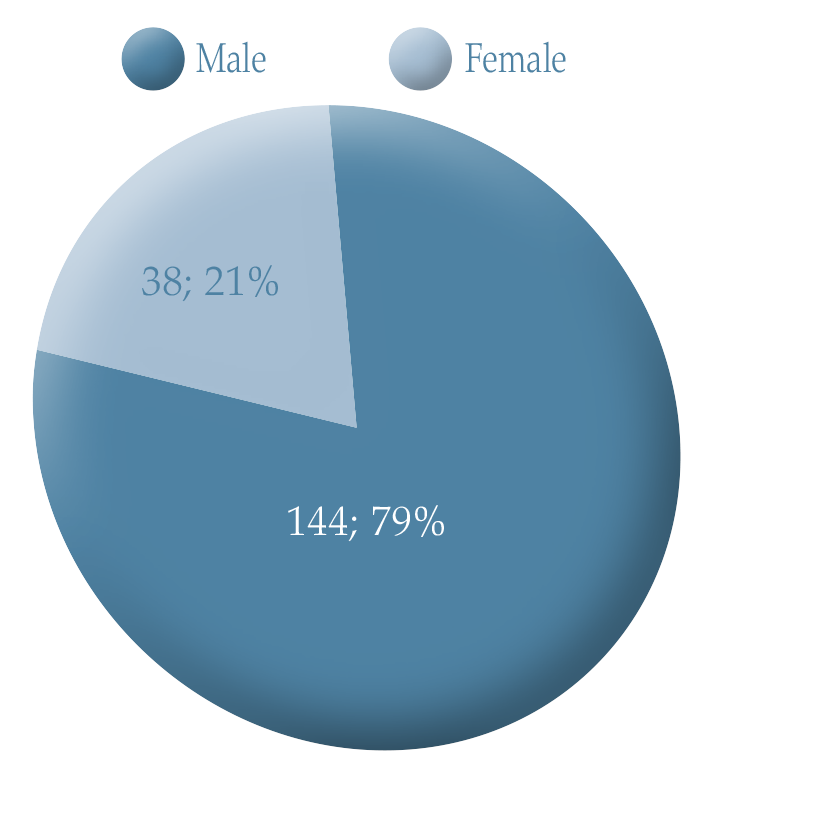
Figure 4. Gender breakdown of participants in the pilot community TWOC.
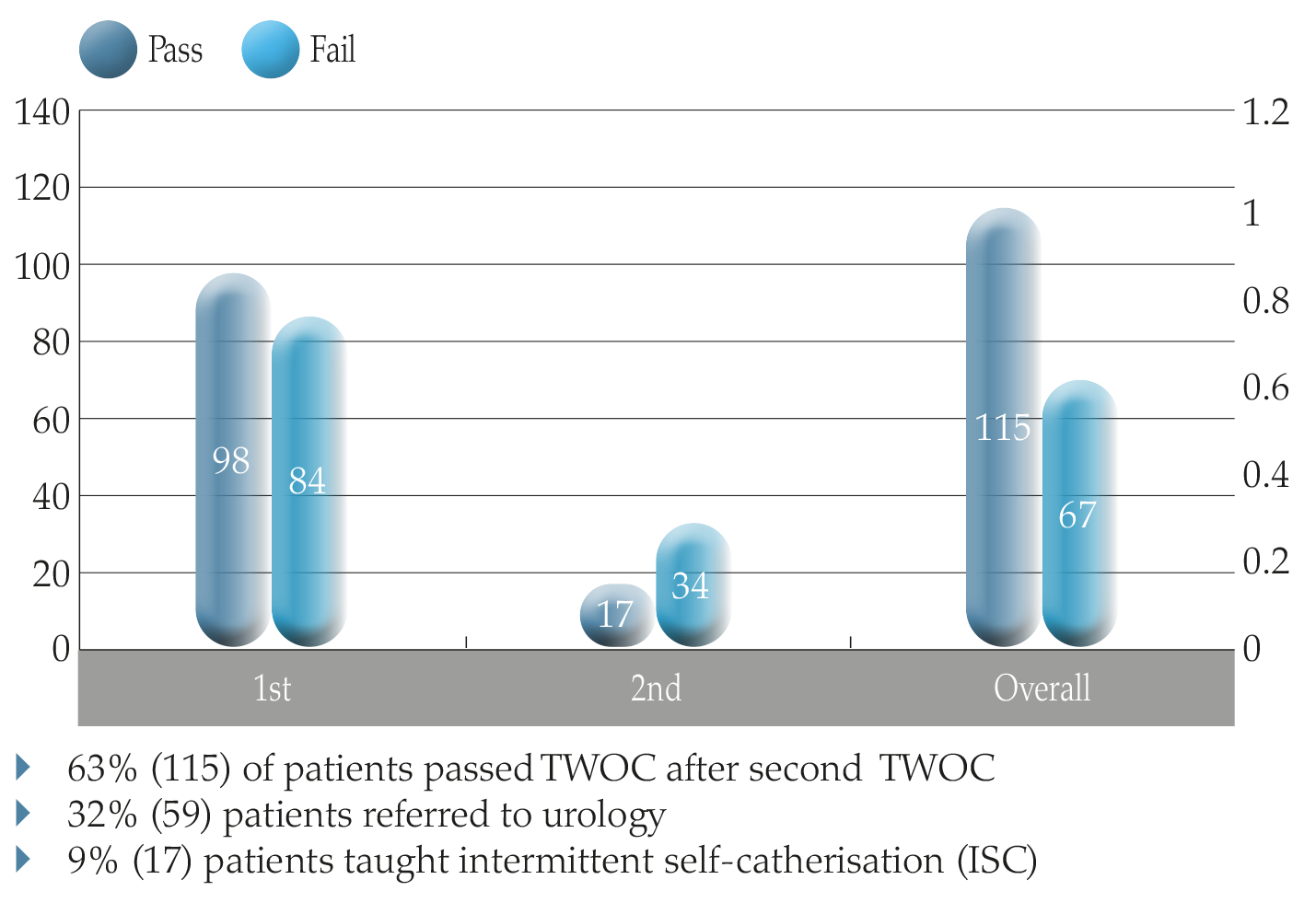
Figure 6. Outcomes of pilot TWOC in the community.
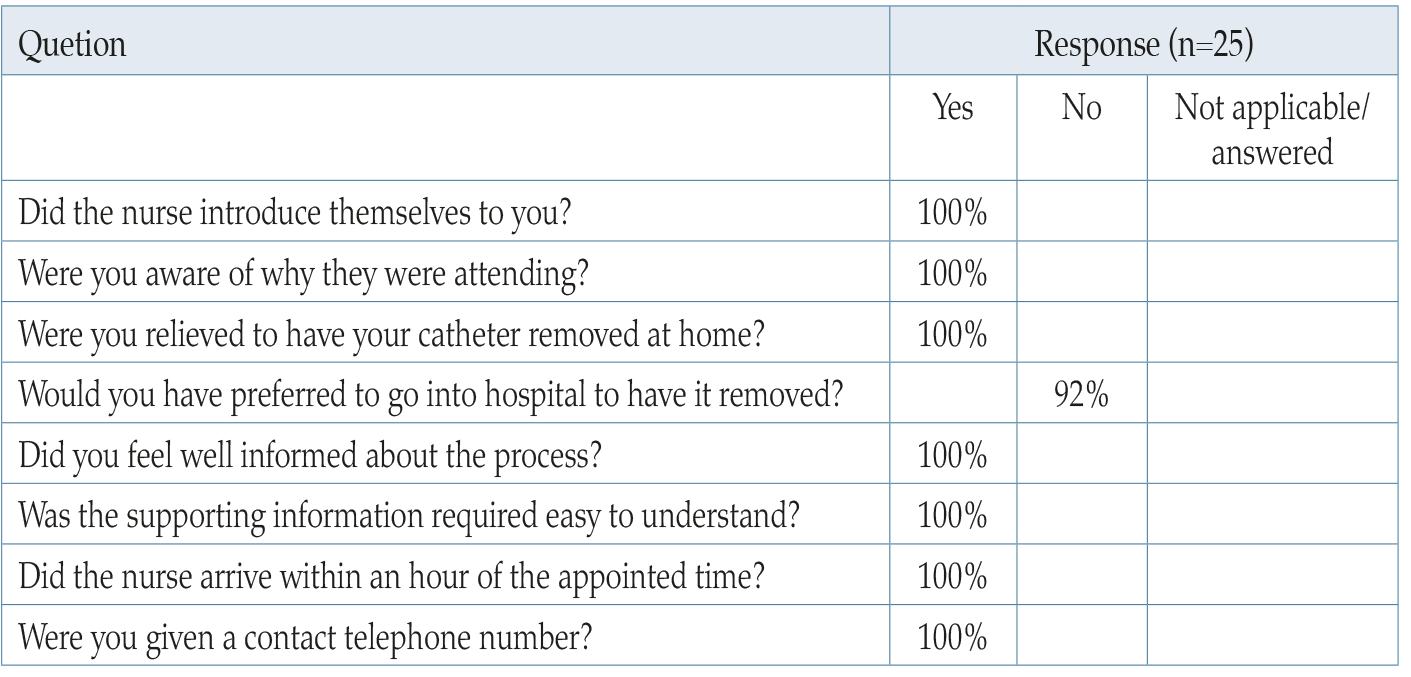
Table 2. Patient experience survey.
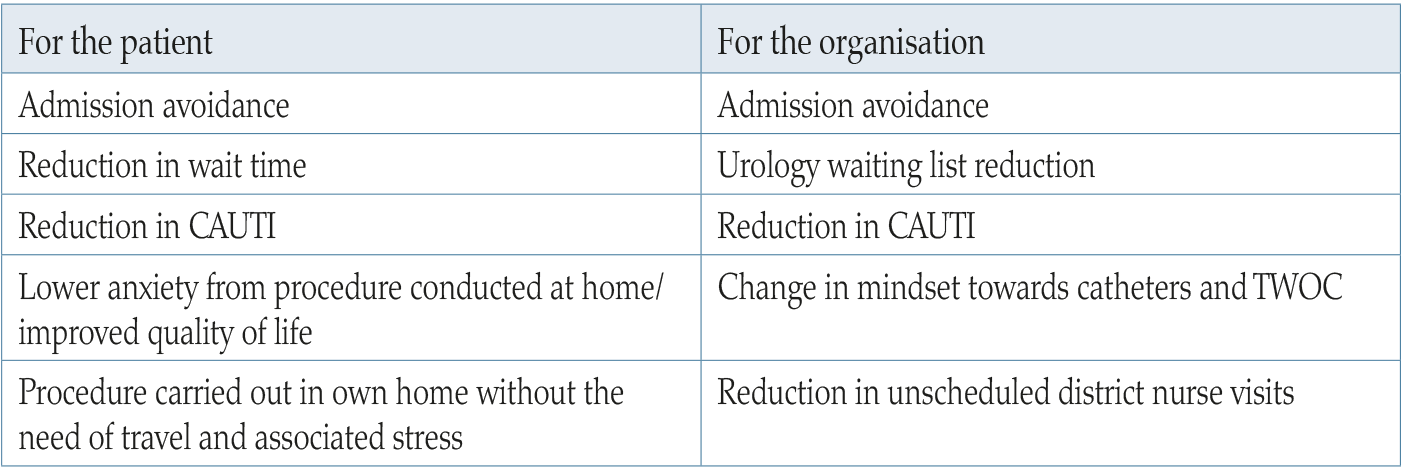
Table 3. Benefits.
References
Adams D, Bucior H, Day G, Rimmer J (2012) HOUDINI: Make that urinary catheter disappear — nurse-led protocol. J Infect Prevent 13(2): 44–46
Cavanagh C (2018) Introducing a referral pathway and proforma for trial without catheter. Br J Nurs 27(Sup6): S8–S9
Colemeadow J, Hasheim T, Batura D (2018) Trial without catheter. Br J Hosp Med 79(3): C42–C44
Dawson C, Gallo M, Prevc K (2017) TWOC around the clock: a multimodal approach to improving catheter care. J Infect Prevent 18(2): 57–64
Elwell R (2015) Developing a nurseled integrated ‘red legs’ service. Br J Community Nurs 19(1): 12, 14–19
Feneley R, Hopley I, Wells P (2015) Urinary catheters: history, current status, adverse events and research agenda. J Med Eng Technol 39(8): 459–70
Gage H, Avery M, Flannery C, Williams P, Fader M (2017) Community prevalence of long term urinary catheters use in England. Neurourol Urodyn 36(2): 293–6
Harvard (2014) cited in Colemeadow J (2018) Trial without catheter. Br J Hosp Med 79(3)
A healthier Wales: long term plan for health and social care (2021) Available online: https://gov.wales/healthier-wales-long-term-plan-health-and-social-care
Heavens K (2018) Trial without catheter referral pathways: Using district nursing services. Br J Nurs 27(sup6)
Holroyd S (2020) Trial without catheter; what is best practice? J Community Nurs 34(2): 60–7
Loveday HP, Wilson JA, Pratt RJ, et al (2014) epic 3: epic3: national evidencebased guidelines for preventing healthcare-associated infections in NHS hospitals in England. J Hosp Infect 86(Suppl 1): S1–70
Mengis J, Nicolini D (2010) Root cause analysis in clinical adverse events. Nurs Manag 16(9): 16–20
National Patient Safety Agency (2004) Root cause analysis toolkit. Cited in Mengis J, Davide N (2010) Root cause analysis in clinical adverse events. Nurs Manag 16(9): 16–20
Nazarko L (2020) Trial without catheters in community setting. Independent Nurse 11: 18–22
Pearson L (2018) Reducing the local use of indwelling urinary catheters in Wolverhampton. Br J Nurs 27(Sup6): S10–S11
Reid S, Brocksom J, Hamid R, et al (2021) British Association of Urological Surgeons (BAUS) and Nurses (BAUN) consensus document: management of the complications of long-term indwelling catheters. BJU Int 128: 667–77
Robinson J (2005) Removing indwelling catheters: trial without catheter in the community. Br J Community Nurs 10(12): 553–7
Tay IJ, Lyons H, Karrouze I, Taylor C, Khan AH, Thompson PM (2016) Impact of the lack of community catheter care services on the emergency department. BJU Int 118(2): 32734
Warrilow M, Williams D, Guest J (2004) The introduction of a trial without catheter model in primary care. Br J Nurs 13(17): 1035–40
Yatim J ,Wong K, Ling M, Tan K, Hockenberry M (2016) A nurse-driven process for timely removal of urinary catheters. Int J Urol Nurs 10(3): 167–72
This piece was first published in the Journal of Community Nursing. To cite this article use: Logan K, Coghlan V (2022) Transforming trial without catheter service provision. J Community Nurs 36(3): 43-50