

Figure 1
RushingToTheToiletPoster-Final.jpg)
Figure 2
Figure 3
Figure 4
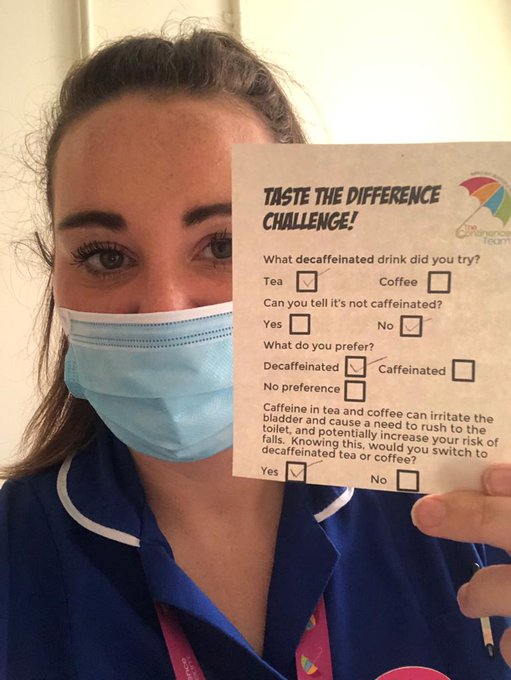
Figure 5. Sarah with the patient feedback form.
If you are interested in delivering your own ‘taste the difference challenge’, then Sarah Coombes, Continence Nurse Specialist at UHL, would love to hear from you.
Email: sarah.j.coombes@uhl-tr.nhs.uk, for further information and a resource pack to get you started.

Email: sarah.j.coombes@uhl-tr.nhs.uk, for further information and a resource pack to get you started.
References
Behling M, Winters B (2021) Methods to stop caffeine use and minimize caffeine withdrawal symptoms in the state of caffeine dependence: a literature review. Available online: https://scholarsarchive.byu.edu/cgi/viewcontent.cgi?article=1363&context=studentpub
Evatt DP, Juliano L, Griffiths R (2016) A brief manualized treatment for problematic caffeine use: a randomized control trial. J Consult Clin Psychol 84(2): 113-121
Jura YH, Townsend MK, Curhan GC, Resnick NM, Grodstein F (2011) Caffeine intake, and the risk of stress, urgency and mixed urinary incontinence. J Urology 185(5): 1775-80
Le Berre M, Presse N, Morin M, et al (2020) What do we really know about the role of caffeine on urinary tract symptoms? A scoping review on caffeine consumption and lower urinary tract symptoms in adults, Neurourol Urodyn 39(5): 1217-1233
NHS inform (2021) Looking after your bones. Available online: https://www.nhsinform.scot/healthy-living/preventing-falls/keeping-well/looking-after-your-bones
Ogeil RP, Phillips JG (2015) Commonly used stimulants: sleep problems, dependence and psychological distress. Drug Alcohol Depend 153: 145-151
Roggeman S, Weiss JP, Van Laecke E, et al (2020) The role of lower urinary tract symptoms in fall risk assessment tools in hospitals: a review. F1000Research, 9: 1-8
Evatt DP, Juliano L, Griffiths R (2016) A brief manualized treatment for problematic caffeine use: a randomized control trial. J Consult Clin Psychol 84(2): 113-121
Jura YH, Townsend MK, Curhan GC, Resnick NM, Grodstein F (2011) Caffeine intake, and the risk of stress, urgency and mixed urinary incontinence. J Urology 185(5): 1775-80
Le Berre M, Presse N, Morin M, et al (2020) What do we really know about the role of caffeine on urinary tract symptoms? A scoping review on caffeine consumption and lower urinary tract symptoms in adults, Neurourol Urodyn 39(5): 1217-1233
NHS inform (2021) Looking after your bones. Available online: https://www.nhsinform.scot/healthy-living/preventing-falls/keeping-well/looking-after-your-bones
Ogeil RP, Phillips JG (2015) Commonly used stimulants: sleep problems, dependence and psychological distress. Drug Alcohol Depend 153: 145-151
Roggeman S, Weiss JP, Van Laecke E, et al (2020) The role of lower urinary tract symptoms in fall risk assessment tools in hospitals: a review. F1000Research, 9: 1-8