

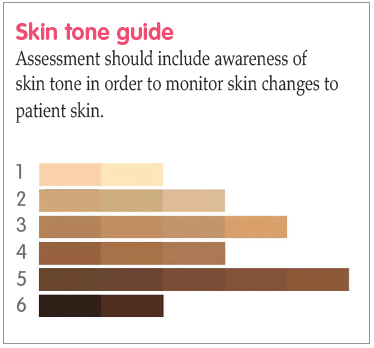
Figure 1. Skin tone tool (adapted from Ho and Robinson, 2015).

Figure 2. Erythema is clearly visible in skin type 1.

Figure 3. Erythema is less obvious in skin type 4.

Patient A: at initial tissue viability assessment

Patient A: four weeks later

Patient A: eight weeks later

Patient A: 12 weeks later

Patient B: at initial TV assessment

Patient B: four weeks later

Patient C: at initial TV assessment
Patient C: eight weeks later

Patient C: 12 weeks later
References
Beeckman D, Campbell J, Campbell K, et al (2015) Proceedings of the Global IAD Expert Panel. Incontinence Associated Dermatitis: Moving Prevention Forward. Wounds International, London
Beeckman D, Van den Bussche K, Alves P, et al (2018) Towards an international language for incontinence-associated dermatitis (IAD): design and evaluation of psychometric properties of the Ghent Global IAD Categorization Tool (GLOBIAD) in 30 countries. Br J Dermatol 178(6): 1331–40
Cutting K, Westgate SJ (2012) The use of wound cleansing solutions in chronic wounds. Wounds UK 8: 130–3
Dhoonmoon L, Dyer M (2020) Improving leg ulcer care in the community. J Community Nurs 34(6): 40–4
Fletcher J, Beeckman D, Boyles A (2020) International Best Practice Recommendations. Prevention and management of moistureassociated skin damage (MASD). Wounds International. Available online: www.woundsinternationalcom
Francis K (2019) Damage control: Differentiating incontinence-associated dermatitis from pressure injury. Nursing 14(6): 18–25
Glass GF Jr, Goh CCK, Cheong RQ, Ong ZL, Khong PCB, Chan EY (2021) Effectiveness of skin cleanser and protectant regimen on incontinenceassociated dermatitis outcomes in acute care patients: A cluster randomised trial. Int Wound J 18(6): 862–73 (published correction appears in Int Wound J [2022] 19(7): 1955)
Gov.UK (2021) Ethnicity facts and figures. Available online: www.ethnicity-factsfigures.service.gov.uk/
Gray M, Black JM, Baharestani MM, et al (2011) Moisture-associated skin damage: overview and pathophysiology. J Wound Ostomy Continence Nurs 38(3): 233–41
Green M, Kashetsky N, Feschuk A, Maibach HI (2022) Transepidermal water loss (TEWL): environment and pollution - A systematic review. Skin Health Dis 2(2): e104
Gupta V, Sharma VK (2019) Skin typing: Fitzpatrick grading and others. Clin Dermatol 37(5): 430–6
Ho BK, Robinson JK (2015) Color bar tool for skin type self-identification: A crosssectional study. J Am Acad Dermatol 73(2): 312–3
Lopez-Ojeda W, Pandey A, Alhajj M, et al (2022) Anatomy, Skin (Integument) [Updated 2022 Oct 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan. Available online: www.ncbi.nlm.nih.gov/books/NBK441980/
Meyer I, Richter HE (2015) Impact of fecal incontinence and its treatment on quality of life in women. Womens Health (Lond) 11(2): 225–38
Moore Z, Bell T, Carville K, et al (2015) International Best Practice Statement: Optimising patient involvement in wound management. Wounds International, London
Mukwende M (2020) Mind the Gap: a clinical handbook of signs and symptoms in black and brown skin. Wounds UK 16(3): 16
Nakagami G, Sanada H, Kitagawa A, et al (2006) Incontinence induces stratum corneum vulnerability and impairs the skin barrier function in the perianal region. Dermatology 213(4): 293–9
NHS England (2018) Excellence in Continence Care. Available online: www.england.nhs.uk/wp-content/uploads/2018/07/excellence-in-continence-care.pdf
Nijhawan R, Alexis A (2011) Practical approaches to medical and cosmetic dermatology in skin of color patients. Expert Rev Dermatol 6: 175–87
Norton C, Thomas L, Hill J (2007) Guideline Development Group. Management of faecal incontinence in adults: summary of NICE guidance. BMJ 334(7608): 1370–71
Vanscheidt W, Harding K, Teot L, Siebert J (2012) Effectiveness and tissue compatibility of a 12-week treatment of chronic venous leg ulcers with an octenidine based antiseptic — a randomized, double-blind controlled study. Int Wound J 9(3): 316–23
Waller S, Cole N (2023) Versatility of a skin protectant ointment in managing moisture-associated skin damage caused by incontinence. Wounds UK 19(1): 58–63
Woo KY, Beeckman D, Chakravarthy D (2017) Management of moistureassociated skin damage: a scoping review. Adv Skin Wound care 30(11): 494–501
Wounds UK (2021) Best Practice Statement: Addressing skin tone bias in wound care: assessing signs and symptoms in people with dark skin tones. Wounds UK, London. Available online: www.wounds-uk.com
Woodward S, Norton C (2020) New study into treatment and prevention of incontinence-associated dermatitis. King’s College, London. Available online: www.kcl.ac.uk/news/new-studyinto-treatment-and-prevention-ofincontinence-associated-dermatitis
Young T (2017) Back to basics: understanding moisture-associated skin damage. Wounds UK 13(2): 56–65
Beeckman D, Van den Bussche K, Alves P, et al (2018) Towards an international language for incontinence-associated dermatitis (IAD): design and evaluation of psychometric properties of the Ghent Global IAD Categorization Tool (GLOBIAD) in 30 countries. Br J Dermatol 178(6): 1331–40
Cutting K, Westgate SJ (2012) The use of wound cleansing solutions in chronic wounds. Wounds UK 8: 130–3
Dhoonmoon L, Dyer M (2020) Improving leg ulcer care in the community. J Community Nurs 34(6): 40–4
Fletcher J, Beeckman D, Boyles A (2020) International Best Practice Recommendations. Prevention and management of moistureassociated skin damage (MASD). Wounds International. Available online: www.woundsinternationalcom
Francis K (2019) Damage control: Differentiating incontinence-associated dermatitis from pressure injury. Nursing 14(6): 18–25
Glass GF Jr, Goh CCK, Cheong RQ, Ong ZL, Khong PCB, Chan EY (2021) Effectiveness of skin cleanser and protectant regimen on incontinenceassociated dermatitis outcomes in acute care patients: A cluster randomised trial. Int Wound J 18(6): 862–73 (published correction appears in Int Wound J [2022] 19(7): 1955)
Gov.UK (2021) Ethnicity facts and figures. Available online: www.ethnicity-factsfigures.service.gov.uk/
Gray M, Black JM, Baharestani MM, et al (2011) Moisture-associated skin damage: overview and pathophysiology. J Wound Ostomy Continence Nurs 38(3): 233–41
Green M, Kashetsky N, Feschuk A, Maibach HI (2022) Transepidermal water loss (TEWL): environment and pollution - A systematic review. Skin Health Dis 2(2): e104
Gupta V, Sharma VK (2019) Skin typing: Fitzpatrick grading and others. Clin Dermatol 37(5): 430–6
Ho BK, Robinson JK (2015) Color bar tool for skin type self-identification: A crosssectional study. J Am Acad Dermatol 73(2): 312–3
Lopez-Ojeda W, Pandey A, Alhajj M, et al (2022) Anatomy, Skin (Integument) [Updated 2022 Oct 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan. Available online: www.ncbi.nlm.nih.gov/books/NBK441980/
Meyer I, Richter HE (2015) Impact of fecal incontinence and its treatment on quality of life in women. Womens Health (Lond) 11(2): 225–38
Moore Z, Bell T, Carville K, et al (2015) International Best Practice Statement: Optimising patient involvement in wound management. Wounds International, London
Mukwende M (2020) Mind the Gap: a clinical handbook of signs and symptoms in black and brown skin. Wounds UK 16(3): 16
Nakagami G, Sanada H, Kitagawa A, et al (2006) Incontinence induces stratum corneum vulnerability and impairs the skin barrier function in the perianal region. Dermatology 213(4): 293–9
NHS England (2018) Excellence in Continence Care. Available online: www.england.nhs.uk/wp-content/uploads/2018/07/excellence-in-continence-care.pdf
Nijhawan R, Alexis A (2011) Practical approaches to medical and cosmetic dermatology in skin of color patients. Expert Rev Dermatol 6: 175–87
Norton C, Thomas L, Hill J (2007) Guideline Development Group. Management of faecal incontinence in adults: summary of NICE guidance. BMJ 334(7608): 1370–71
Vanscheidt W, Harding K, Teot L, Siebert J (2012) Effectiveness and tissue compatibility of a 12-week treatment of chronic venous leg ulcers with an octenidine based antiseptic — a randomized, double-blind controlled study. Int Wound J 9(3): 316–23
Waller S, Cole N (2023) Versatility of a skin protectant ointment in managing moisture-associated skin damage caused by incontinence. Wounds UK 19(1): 58–63
Woo KY, Beeckman D, Chakravarthy D (2017) Management of moistureassociated skin damage: a scoping review. Adv Skin Wound care 30(11): 494–501
Wounds UK (2021) Best Practice Statement: Addressing skin tone bias in wound care: assessing signs and symptoms in people with dark skin tones. Wounds UK, London. Available online: www.wounds-uk.com
Woodward S, Norton C (2020) New study into treatment and prevention of incontinence-associated dermatitis. King’s College, London. Available online: www.kcl.ac.uk/news/new-studyinto-treatment-and-prevention-ofincontinence-associated-dermatitis
Young T (2017) Back to basics: understanding moisture-associated skin damage. Wounds UK 13(2): 56–65