

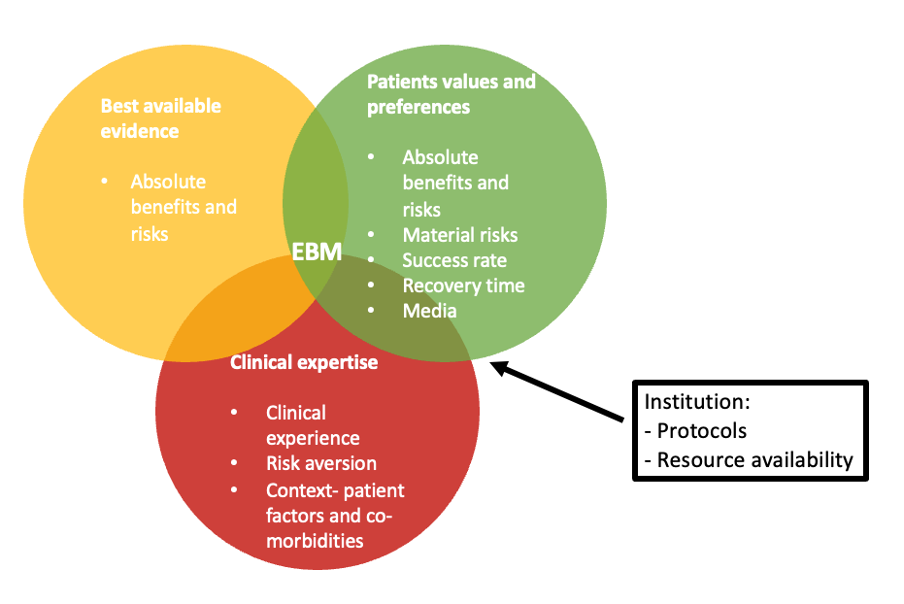
Figure 1. Evidence-based medicine (EBM) triad
Table 2. Surgical procedures included in patient decision aids for the National Institute for Health and Care Excellence (2019) guidance
| Surgical options | ||||
| Condition | Uterine preserving | Non-uterine preserving | ||
| Uterine prolapse | Vaginal sacrospinous hysteropexy with sutures | Manchester repair | Sacrohysteropexy with mesh | Vaginal hysterectomy |
| Vaginal vault prolapse | Sacrospinous fixation of vault | Sacrocolpopexy with mesh | ||
| Stress urinary incontinence | Bulking agents | Colposuspension | Rectus fascial sling | Retropubic mesh tapes |
Qualitative research evaluating the role of the clinician in the decision-making process regarding surgery for stress urinary incontinence (Cox, 2019) found that both patient characteristics and clinician preferences were significant influencing factors. Patient characteristics that influenced clinicians’ interpretation of procedural benefits and risk included clinical characteristics such as age, body mass index, medical comorbidities, symptom severity, impact on quality of life and the presence of co-existing pelvic organ prolapse or urethra hypermobility. Clinician preferences influencing decision making included surgical familiarity and procedural preference, risk aversion, institutional resource availability and individual interpretation of clinical evidence. Overall, this can lead to a difference in counselling despite patient decision aids.
It is important to note that clinician preferences may also influence surgical technique and outcomes. This was highlighted in the Variation in Surgical Technique study (VaST) (Fairclough et al, 2024) which demonstrated that in anterior pelvic organ prolapse surgery, differences in fascial dissection (Figure 2), fascial repair and vaginal skin closure techniques affected both subjective (measured using the Pelvic Organ Prolapse Symptom Score (POP-SS)) and objective outcomes (assessed using POP-Q measurement Ba at 12 months).
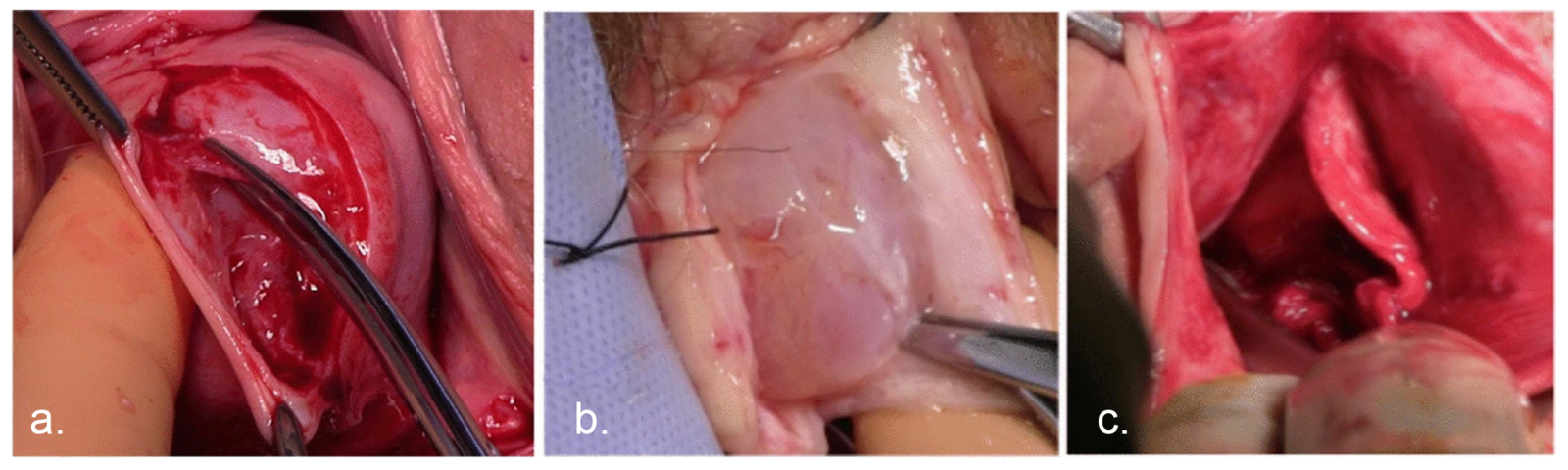
Figure 2. Photographic illustrations of the methods of fascial dissection. A. Superficial dissection. B. Deep dissection. C. Fascial flap dissection. Reproduced by permission from Fairclough et al (2024).
It is important to note that clinician preferences may also influence surgical technique and outcomes. This was highlighted in the Variation in Surgical Technique study (VaST) (Fairclough et al, 2024) which demonstrated that in anterior pelvic organ prolapse surgery, differences in fascial dissection (Figure 2), fascial repair and vaginal skin closure techniques affected both subjective (measured using the Pelvic Organ Prolapse Symptom Score (POP-SS)) and objective outcomes (assessed using POP-Q measurement Ba at 12 months).
Figure 2. Photographic illustrations of the methods of fascial dissection. A. Superficial dissection. B. Deep dissection. C. Fascial flap dissection. Reproduced by permission from Fairclough et al (2024).
Patient decision making
The risks and benefits of surgery are valued differently by patients. Therefore, it is vital that thorough discussion of the likelihood of a potential outcome occurring is explained in a clear and understandable way, taking into account the patient’s values and personal context. Table 3 details the risks outlined by the British Society of Urogynaecology and the Royal College of Obstetricians & Gynaecologists for procedures offered to treat stress urinary incontinence and pelvic organ prolapse, including colposuspension and vaginal hysterectomy.References
Alio AP, Merrell L, Roxburgh K et al (2011) The psychosocial impact of vesico-vaginal fistula in Niger. Arch Gynecol Obstet. 284(2):371–8. https://doi.org/10.1007/s00404-010-1652-5
Anandan PK, Sivakumar S (2020) An assessment of the factors affecting surgical decision making: a multi institutional study. International Surgery Journal. 7(4):1138–1142. https://doi.org/10.18203/2349-2902.isj20201388
Anger JT, Lee UJ, Mittal BM, Pollard ME, Tarnay CM, Maliski S, Rogers RG (2012) Health literacy and disease understanding among aging women with pelvic floor disorders. Female Pelvic Med Reconstr Surg. 18(6):340-3. https://doi.org/10.1097/SPV.0b013e31826fb8d3
Athey R, Bugeja R, Jones G, Jha S (2025) Impact of patients decision aids on shared decision-making and patient satisfaction prior to pelvic floor surgery. BJOG. 132(7):918-926. https://doi.org/10.1111/1471-0528.18103
Brehaut JC, O'Connor AM, Wood TJ, Hack TF, Siminoff L, Gordon E, Feldman-Stewart D (2003) Validation of a decision regret scale. Med Decis Making. 23(4):281-92. https://doi.org/10.1177/0272989X03256005
British Society of Urogynaecology (2018) Colposuspension for stress urinary incontinence. https://bsug.org.uk/budcms/includes/kcfinder/upload/files/Colposuspension%20Apr%202018.pdf (accessed 18 December 2025)
Bugeja R, Athey R, Jha S (2025) Patient decision aids for pelvic floor surgery and impact on decisional conflict. BJOG. 132(12):1817-1822. https://doi.org/10.1111/1471-0528.18311
Cox S (2019) A study of factors that influence the choice of primary surgical procedure for stress urinary incontinence from the perspective of patients and clinicians. Thesis for Master of Philosophy. https://research.manchester.ac.uk/en/studentTheses/a-study-of-factors-that-influence-the-choice-of-primary-surgical-/ (accessed 5 January 2026)
Cumberlege J (2020) First Do No Harm: The report of the Independent Medicines and Medical Devices Safety Review. https://www.immdsreview.org.uk/downloads/IMMDSReview_Web.pdf (accessed 18 December 2025)
De Oliveira GS Jr, McCarthy RJ, Wolf MS, Holl J (2015) The impact of health literacy in the care of surgical patients: a qualitative systematic review. BMC Surg. 15:86. https://doi.org/10.1186/s12893-015-0073-6
Dwyer L, Weaver E, Rajai A, Cox S, Reid F (2020) "Voice your choice": a study of women's choice of surgery for primary stress urinary incontinence. Int Urogynecol J. 31(4):769-777. https://doi.org/10.1007/s00192-019-04202-6
El-Hamamsy D, Parmar C, Shoop-Worrall S, Reid FM (2022) Public understanding of female genital anatomy and pelvic organ prolapse (POP); a questionnaire-based pilot study. Int Urogynecol J. 33(2):309-318. https://doi.org/10.1007/s00192-021-04727-9
Fairclough E, Segar J, Breeman S, Smith A, Myers J, Reid F (2024) Does variation of surgical technique affect native tissue anterior pelvic organ prolapse repair outcomes? Int Urogynecol J. 35(1):51-58. https://doi.org/10.1007/s00192-023-05584-4
Ferrari A, Bellè N, Giannini A, Simoncini T, Vainieri M (2024) Determinants of women's preferences for surgical versus conservative management for pelvic organ prolapse: a survey-based study from Italy. BMJ Open. 14(7):e084034. https://doi.org/10.1136/bmjopen-2024-084034
Fialkow MF, Newton KM, Lentz GM, Weiss NS (2008) Lifetime risk of surgical management for pelvic organ prolapse or urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct. 19(3):437-40. https://doi.org/10.1007/s00192-007-0459-9
Gunaratnam C, Bernstein M (2018) Factors affecting surgical decision-making-a qualitative study. Rambam Maimonides Med J. 9(1):e0003. https://doi.org/10.5041/RMMJ.10324
Haylen BT, de Ridder D, Freeman RM et al; International Urogynecological Association; International Continence Society (2010) An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn. 29(1):4-20. https://doi.org/10.1002/nau.20798
Hilton P (2012) Urogenital fistula in the UK: a personal case series managed over 25 years. BJU Int. 110(1):102-10. https://doi.org/10.1111/j.1464-410X.2011.10630.x
Kiyosaki K, Ackerman AL, Histed S et al (2012) Patients' understanding of pelvic floor disorders: what women want to know. Female Pelvic Med Reconstr Surg. 18(3):137-42. https://doi.org/10.1097/SPV.0b013e318254f09c
Montgomery v Lanarkshire Health Board [2015] UKSC/2013/0136
National Institute for Health and Care Excellence (2019) Urinary incontinence and pelvic organ prolapse in women: management. NICE guideline [NG123]. https://www.nice.org.uk/guidance/ng123 (accessed 18 December 2025)
O'Connor AM (1995) Validation of a decisional conflict scale. Med Decis Making. 15(1):25-30. https://doi.org/10.1177/0272989X9501500105
Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL (1997) Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol. 89(4):501-6. https://doi.org/10.1016/S0029-7844(97)00058-6
Ong HL, Sokolova I, Bekarma H, Curtis C, Macdonald A, Agur W; NHS Ayrshire & Arran Continence Multidisciplinary Team (2019) Development, validation and initial evaluation of patient-decision aid (SUI-PDA©) for women considering stress urinary incontinence surgery. Int Urogynecol J. 30(12):2013-2022. https://doi.org/10.1007/s00192-019-04047-z
Ownby RL, Acevedo A, Goodman K, Caballero J, Waldrop-Valverde D (2015) Health literacy predicts participant understanding of orally-presented informed consent information. Clin Res Trials. 1(1):15-19. https://doi.org/10.15761/CRT.1000105
Royal College of Obstetricians & Gynaecologists (2009) Vaginal Surgery For Prolapse (Consent Advice No. 5). https://www.rcog.org.uk/media/sx1fcbt0/ca5-15072010.pdf (accessed 5 January 2026)
Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS (1996) Evidence based medicine: what it is and what it isn't. BMJ. 312(7023):71-2. https://doi.org/10.1136/bmj.312.7023.71
Schulten SFM, Essers B, Notten KJB et al (2023) Patient's preference for sacrospinous hysteropexy or modified Manchester operation: A discrete choice experiment. BJOG. 130(1):99-106. https://doi.org/10.1111/1471-0528.17280
Simpson RM, Knowles E, O'Cathain A (2020) Health literacy levels of British adults: a cross-sectional survey using two domains of the Health Literacy Questionnaire (HLQ). BMC Public Health. 20(1):1819. https://doi.org/10.1186/s12889-020-09727-w
Sridhar S, King C (2025) Impact of social media on patient expectations and decision-making in gynecology. Curr Opin Obstet Gynecol. 37(4):261-267. https://doi.org/10.1097/GCO.0000000000001030
Stacey D, Légaré F, Lewis K et al (2024) Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 1:CD001431. https://doi.org/10.1002/14651858.CD001431.pub6
Sun Q (2004) Predicting Downstream Effects of High Decisional Conflict: Meta-analyses of the Decisional Conflict Scale. University of Ottawa (Canada) Dissertations & Theses. https://ruor.uottawa.ca/items/40b8ee93-a937-451d-9975-827c46650e67/full (accessed 5 January 2026)
Sutherland L (2021) The right of patients to make autonomous choices: Montgomery v Lanarkshire Health Board: a landmark decision on information disclosure to patients in the UK. Int Urogynecol J. 32(7):2005-2010. https://doi.org/10.1007/s00192-021-04882-z
Walton T (2020) Material risk: a review of informed consent in the UK. Orthopaedics and Trauma. 34:131–134. https://doi.org/10.1016/j.mporth.2020.03.005
Williams N, Ogden J (2004) The impact of matching the patient's vocabulary: a randomized control trial. Fam Pract. 21(6):630-5. https://doi.org/10.1093/fampra/cmh610
Wright JP, Edwards GC, Goggins K et al (2018) Association of health literacy with postoperative outcomes in patients undergoing major abdominal surgery. JAMA Surg. 153(2):137-142. https://doi.org/10.1001/jamasurg.2017.3832
Anandan PK, Sivakumar S (2020) An assessment of the factors affecting surgical decision making: a multi institutional study. International Surgery Journal. 7(4):1138–1142. https://doi.org/10.18203/2349-2902.isj20201388
Anger JT, Lee UJ, Mittal BM, Pollard ME, Tarnay CM, Maliski S, Rogers RG (2012) Health literacy and disease understanding among aging women with pelvic floor disorders. Female Pelvic Med Reconstr Surg. 18(6):340-3. https://doi.org/10.1097/SPV.0b013e31826fb8d3
Athey R, Bugeja R, Jones G, Jha S (2025) Impact of patients decision aids on shared decision-making and patient satisfaction prior to pelvic floor surgery. BJOG. 132(7):918-926. https://doi.org/10.1111/1471-0528.18103
Brehaut JC, O'Connor AM, Wood TJ, Hack TF, Siminoff L, Gordon E, Feldman-Stewart D (2003) Validation of a decision regret scale. Med Decis Making. 23(4):281-92. https://doi.org/10.1177/0272989X03256005
British Society of Urogynaecology (2018) Colposuspension for stress urinary incontinence. https://bsug.org.uk/budcms/includes/kcfinder/upload/files/Colposuspension%20Apr%202018.pdf (accessed 18 December 2025)
Bugeja R, Athey R, Jha S (2025) Patient decision aids for pelvic floor surgery and impact on decisional conflict. BJOG. 132(12):1817-1822. https://doi.org/10.1111/1471-0528.18311
Cox S (2019) A study of factors that influence the choice of primary surgical procedure for stress urinary incontinence from the perspective of patients and clinicians. Thesis for Master of Philosophy. https://research.manchester.ac.uk/en/studentTheses/a-study-of-factors-that-influence-the-choice-of-primary-surgical-/ (accessed 5 January 2026)
Cumberlege J (2020) First Do No Harm: The report of the Independent Medicines and Medical Devices Safety Review. https://www.immdsreview.org.uk/downloads/IMMDSReview_Web.pdf (accessed 18 December 2025)
De Oliveira GS Jr, McCarthy RJ, Wolf MS, Holl J (2015) The impact of health literacy in the care of surgical patients: a qualitative systematic review. BMC Surg. 15:86. https://doi.org/10.1186/s12893-015-0073-6
Dwyer L, Weaver E, Rajai A, Cox S, Reid F (2020) "Voice your choice": a study of women's choice of surgery for primary stress urinary incontinence. Int Urogynecol J. 31(4):769-777. https://doi.org/10.1007/s00192-019-04202-6
El-Hamamsy D, Parmar C, Shoop-Worrall S, Reid FM (2022) Public understanding of female genital anatomy and pelvic organ prolapse (POP); a questionnaire-based pilot study. Int Urogynecol J. 33(2):309-318. https://doi.org/10.1007/s00192-021-04727-9
Fairclough E, Segar J, Breeman S, Smith A, Myers J, Reid F (2024) Does variation of surgical technique affect native tissue anterior pelvic organ prolapse repair outcomes? Int Urogynecol J. 35(1):51-58. https://doi.org/10.1007/s00192-023-05584-4
Ferrari A, Bellè N, Giannini A, Simoncini T, Vainieri M (2024) Determinants of women's preferences for surgical versus conservative management for pelvic organ prolapse: a survey-based study from Italy. BMJ Open. 14(7):e084034. https://doi.org/10.1136/bmjopen-2024-084034
Fialkow MF, Newton KM, Lentz GM, Weiss NS (2008) Lifetime risk of surgical management for pelvic organ prolapse or urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct. 19(3):437-40. https://doi.org/10.1007/s00192-007-0459-9
Gunaratnam C, Bernstein M (2018) Factors affecting surgical decision-making-a qualitative study. Rambam Maimonides Med J. 9(1):e0003. https://doi.org/10.5041/RMMJ.10324
Haylen BT, de Ridder D, Freeman RM et al; International Urogynecological Association; International Continence Society (2010) An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn. 29(1):4-20. https://doi.org/10.1002/nau.20798
Hilton P (2012) Urogenital fistula in the UK: a personal case series managed over 25 years. BJU Int. 110(1):102-10. https://doi.org/10.1111/j.1464-410X.2011.10630.x
Kiyosaki K, Ackerman AL, Histed S et al (2012) Patients' understanding of pelvic floor disorders: what women want to know. Female Pelvic Med Reconstr Surg. 18(3):137-42. https://doi.org/10.1097/SPV.0b013e318254f09c
Montgomery v Lanarkshire Health Board [2015] UKSC/2013/0136
National Institute for Health and Care Excellence (2019) Urinary incontinence and pelvic organ prolapse in women: management. NICE guideline [NG123]. https://www.nice.org.uk/guidance/ng123 (accessed 18 December 2025)
O'Connor AM (1995) Validation of a decisional conflict scale. Med Decis Making. 15(1):25-30. https://doi.org/10.1177/0272989X9501500105
Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL (1997) Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol. 89(4):501-6. https://doi.org/10.1016/S0029-7844(97)00058-6
Ong HL, Sokolova I, Bekarma H, Curtis C, Macdonald A, Agur W; NHS Ayrshire & Arran Continence Multidisciplinary Team (2019) Development, validation and initial evaluation of patient-decision aid (SUI-PDA©) for women considering stress urinary incontinence surgery. Int Urogynecol J. 30(12):2013-2022. https://doi.org/10.1007/s00192-019-04047-z
Ownby RL, Acevedo A, Goodman K, Caballero J, Waldrop-Valverde D (2015) Health literacy predicts participant understanding of orally-presented informed consent information. Clin Res Trials. 1(1):15-19. https://doi.org/10.15761/CRT.1000105
Royal College of Obstetricians & Gynaecologists (2009) Vaginal Surgery For Prolapse (Consent Advice No. 5). https://www.rcog.org.uk/media/sx1fcbt0/ca5-15072010.pdf (accessed 5 January 2026)
Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS (1996) Evidence based medicine: what it is and what it isn't. BMJ. 312(7023):71-2. https://doi.org/10.1136/bmj.312.7023.71
Schulten SFM, Essers B, Notten KJB et al (2023) Patient's preference for sacrospinous hysteropexy or modified Manchester operation: A discrete choice experiment. BJOG. 130(1):99-106. https://doi.org/10.1111/1471-0528.17280
Simpson RM, Knowles E, O'Cathain A (2020) Health literacy levels of British adults: a cross-sectional survey using two domains of the Health Literacy Questionnaire (HLQ). BMC Public Health. 20(1):1819. https://doi.org/10.1186/s12889-020-09727-w
Sridhar S, King C (2025) Impact of social media on patient expectations and decision-making in gynecology. Curr Opin Obstet Gynecol. 37(4):261-267. https://doi.org/10.1097/GCO.0000000000001030
Stacey D, Légaré F, Lewis K et al (2024) Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 1:CD001431. https://doi.org/10.1002/14651858.CD001431.pub6
Sun Q (2004) Predicting Downstream Effects of High Decisional Conflict: Meta-analyses of the Decisional Conflict Scale. University of Ottawa (Canada) Dissertations & Theses. https://ruor.uottawa.ca/items/40b8ee93-a937-451d-9975-827c46650e67/full (accessed 5 January 2026)
Sutherland L (2021) The right of patients to make autonomous choices: Montgomery v Lanarkshire Health Board: a landmark decision on information disclosure to patients in the UK. Int Urogynecol J. 32(7):2005-2010. https://doi.org/10.1007/s00192-021-04882-z
Walton T (2020) Material risk: a review of informed consent in the UK. Orthopaedics and Trauma. 34:131–134. https://doi.org/10.1016/j.mporth.2020.03.005
Williams N, Ogden J (2004) The impact of matching the patient's vocabulary: a randomized control trial. Fam Pract. 21(6):630-5. https://doi.org/10.1093/fampra/cmh610
Wright JP, Edwards GC, Goggins K et al (2018) Association of health literacy with postoperative outcomes in patients undergoing major abdominal surgery. JAMA Surg. 153(2):137-142. https://doi.org/10.1001/jamasurg.2017.3832