

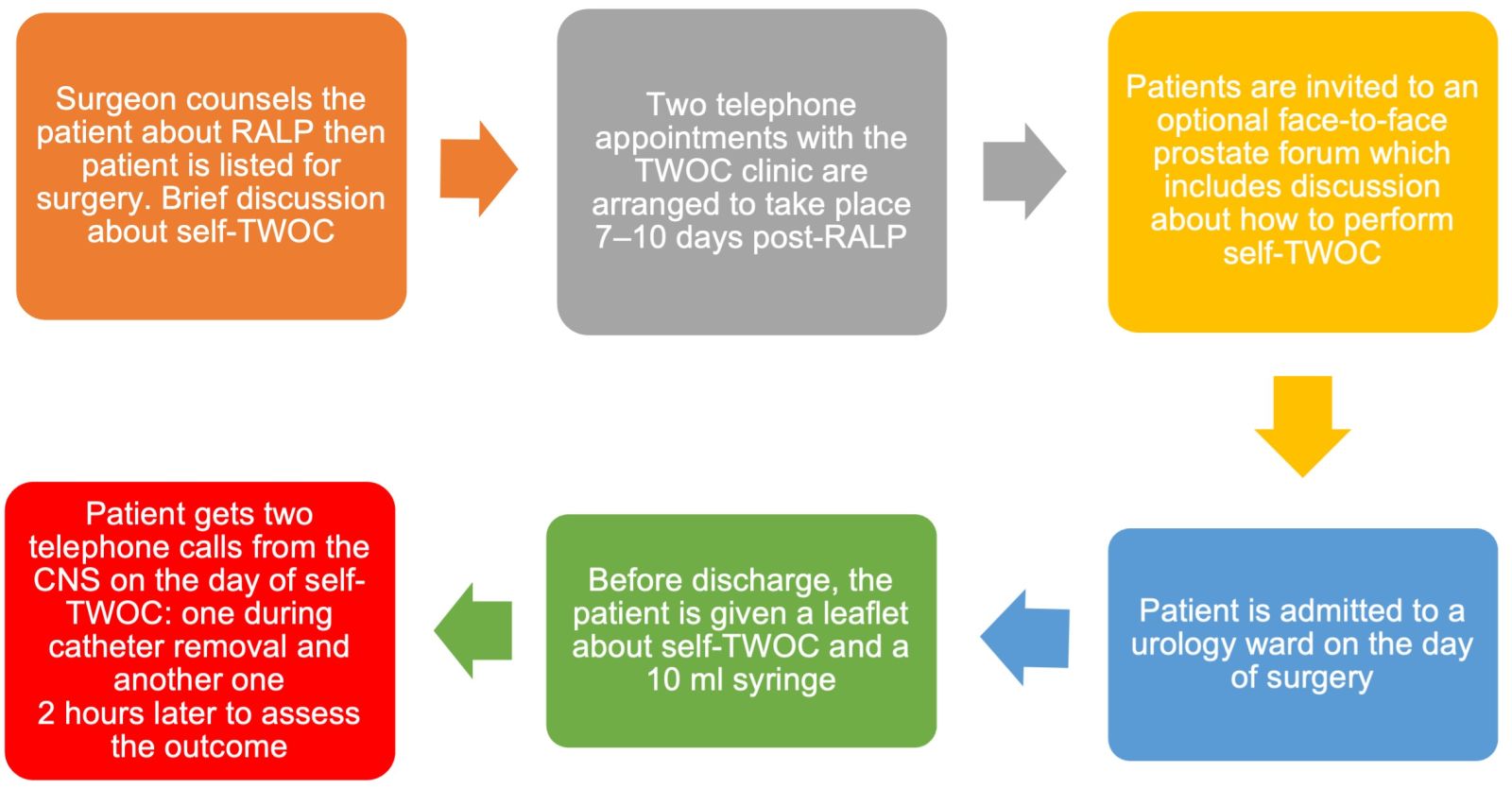
Figure 1. The East Kent Hospitals University Foundation NHS Trust pathway for patients performing self-trial without catheter (TWOC) after a robotic-assisted laparoscopic prostatectomy (RALP). CNS = clinical nurse specialist.
References
Braungart S, Goyal A (2019) Parental home removal of urethral catheters after urological surgery-a prospective benchmarking study. J Pediatr Urol 15(3): 252.e1-252.e4. https://doi.org/10.1016/j.jpurol.2019.03.018
Cancer Research UK (2026) Prostate cancer statistics. https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/prostate-cancer (accessed 16 April 2026)
Christiaans C, van Veen F, Blok B (2025) Patient satisfaction and quality of life in long-term urinary catheter users in the Netherlands. A nationwide survey study. EMJ Urol 13(1): 38–9. https://doi.org/10.33590/emjurol/EZCI7981
Department for Environment, Food & Rural Affairs (2025) Government conversion factors for company reporting of greenhouse gas emissions. https://www.gov.uk/government/collections/government-conversion-factors-for-company-reporting (accessed 7 May 2026)
East Kent Hospitals University Foundation NHS Trust (2024) Robotic-assisted laparoscopic
prostatectomy: Kent and Canterbury Hospital. https://leaflets.ekhuft.nhs.uk/s3/leaflets/robotic-assisted-laparoscopic-prostatectomy-kent-and-canterbury-hospital/6c9c4c78-5cdb-4597-8f6f-3584c6293b34.p1724930721.pdf (accessed 16 April 2026)
HM Revenue & Customs (2026) Advisory fuel rates. https://www.gov.uk/guidance/advisory-fuel-rates (accessed 7 May 2026)
Kwint J, Hoskin L (2023) 7 Findings that could save the NHS money and improve care. https://doi.org/10.3310/nihrevidence_56221 (accessed 16 April 2026)
Lunas JM, Holborn C, Appleyard R et al (2026) Comparison of self-removal and clinic-removal of catheter after robot-assisted laparoscopic prostatectomy. Eur J Oncol Nurs 80: 103072. https://doi.org/10.1016/j.ejon.2025.103072
NHS England (2019) The NHS Long Term Plan. https://www.longtermplan.nhs.uk/ (accessed 7 May 2026)
NHS England (2020) Delivering a ‘Net Zero’ National Health Service. https://www.england.nhs.uk/greenernhs/wp-content/uploads/sites/51/2020/10/delivering-a-net-zero-national-health-service.pdf (accessed 16 April 2026)
NHS England (2026a) Neighbourhood health framework. https://www.gov.uk/government/publications/neighbourhood-health-framework/neighbourhood-health-framework (accessed 8 May 2026)
NHS England (2026b) National Cost Collection for the NHS. https://www.england.nhs.uk/costing-in-the-nhs/national-cost-collection/ (accessed 16 April 2026)
Rahman E, Penev B, Bhatti I et al (2025) Self-urinary catheter removal for urology day cases: a safe, efficient, sustainable, and patient-centred approach. Cureus 17(10): e94256. https://doi.org/10.7759/cureus.94256
Samadi DB (2025) Best treatment options for prostate cancer in 2025. https://roboticoncology.com/post/best-treatment-options-for-prostate-cancer-in-2025 (accessed 16 April 2026)
Saville K, Bewley J (2025) Trial without catheter: an alternative approach. J Community Nurs 39(4): 44–9
Viera C (2023) How to write limitations of the study (with examples). https://www.aje.com/arc/how-to-write-limitations-of-the-study (accessed 16 April 2026)
Cancer Research UK (2026) Prostate cancer statistics. https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/prostate-cancer (accessed 16 April 2026)
Christiaans C, van Veen F, Blok B (2025) Patient satisfaction and quality of life in long-term urinary catheter users in the Netherlands. A nationwide survey study. EMJ Urol 13(1): 38–9. https://doi.org/10.33590/emjurol/EZCI7981
Department for Environment, Food & Rural Affairs (2025) Government conversion factors for company reporting of greenhouse gas emissions. https://www.gov.uk/government/collections/government-conversion-factors-for-company-reporting (accessed 7 May 2026)
East Kent Hospitals University Foundation NHS Trust (2024) Robotic-assisted laparoscopic
prostatectomy: Kent and Canterbury Hospital. https://leaflets.ekhuft.nhs.uk/s3/leaflets/robotic-assisted-laparoscopic-prostatectomy-kent-and-canterbury-hospital/6c9c4c78-5cdb-4597-8f6f-3584c6293b34.p1724930721.pdf (accessed 16 April 2026)
HM Revenue & Customs (2026) Advisory fuel rates. https://www.gov.uk/guidance/advisory-fuel-rates (accessed 7 May 2026)
Kwint J, Hoskin L (2023) 7 Findings that could save the NHS money and improve care. https://doi.org/10.3310/nihrevidence_56221 (accessed 16 April 2026)
Lunas JM, Holborn C, Appleyard R et al (2026) Comparison of self-removal and clinic-removal of catheter after robot-assisted laparoscopic prostatectomy. Eur J Oncol Nurs 80: 103072. https://doi.org/10.1016/j.ejon.2025.103072
NHS England (2019) The NHS Long Term Plan. https://www.longtermplan.nhs.uk/ (accessed 7 May 2026)
NHS England (2020) Delivering a ‘Net Zero’ National Health Service. https://www.england.nhs.uk/greenernhs/wp-content/uploads/sites/51/2020/10/delivering-a-net-zero-national-health-service.pdf (accessed 16 April 2026)
NHS England (2026a) Neighbourhood health framework. https://www.gov.uk/government/publications/neighbourhood-health-framework/neighbourhood-health-framework (accessed 8 May 2026)
NHS England (2026b) National Cost Collection for the NHS. https://www.england.nhs.uk/costing-in-the-nhs/national-cost-collection/ (accessed 16 April 2026)
Rahman E, Penev B, Bhatti I et al (2025) Self-urinary catheter removal for urology day cases: a safe, efficient, sustainable, and patient-centred approach. Cureus 17(10): e94256. https://doi.org/10.7759/cureus.94256
Samadi DB (2025) Best treatment options for prostate cancer in 2025. https://roboticoncology.com/post/best-treatment-options-for-prostate-cancer-in-2025 (accessed 16 April 2026)
Saville K, Bewley J (2025) Trial without catheter: an alternative approach. J Community Nurs 39(4): 44–9
Viera C (2023) How to write limitations of the study (with examples). https://www.aje.com/arc/how-to-write-limitations-of-the-study (accessed 16 April 2026)