

THE SECRET LIFE OF CATHETERS
 This 11-module programme consists of short, animated lectures delivered in three to four-hour sessions. Six modules deal with core anatomical themes, the fundamentals of material science and the biology of catheter life. The five further sequential modules cover clinical dimensions of catheter care. The aim of the programme is to ‘iron out’ many of the confusions, myths and misunderstandings that surround catheter care.
This 11-module programme consists of short, animated lectures delivered in three to four-hour sessions. Six modules deal with core anatomical themes, the fundamentals of material science and the biology of catheter life. The five further sequential modules cover clinical dimensions of catheter care. The aim of the programme is to ‘iron out’ many of the confusions, myths and misunderstandings that surround catheter care.All sessions include interactive feedback and self-assessment to help consolidate knowledge gained. In a multiprofessional group setting, training sessions conclude with structured case studies, which are designed to enable reflective learning and sharing experiences across interdisciplinary boundaries.
Course overview
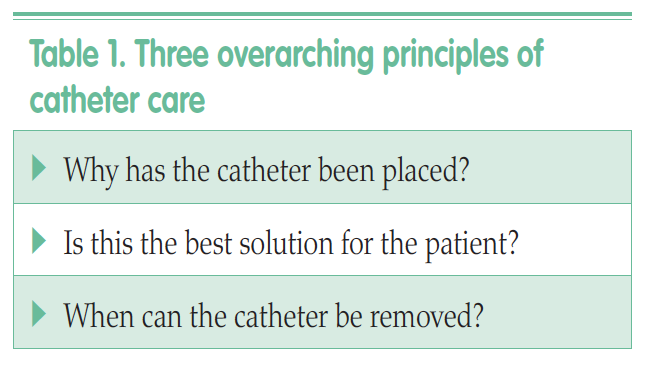
It is beyond the scope of this article to cover all the content, however, what follows is a taster of some key aspects of the course.Module one is an introduction to the course and introduces the three overarching principles of catheter care (Table 1). For those clinicians trained in catheter insertion, the course focuses on eight golden rules (Table 2).
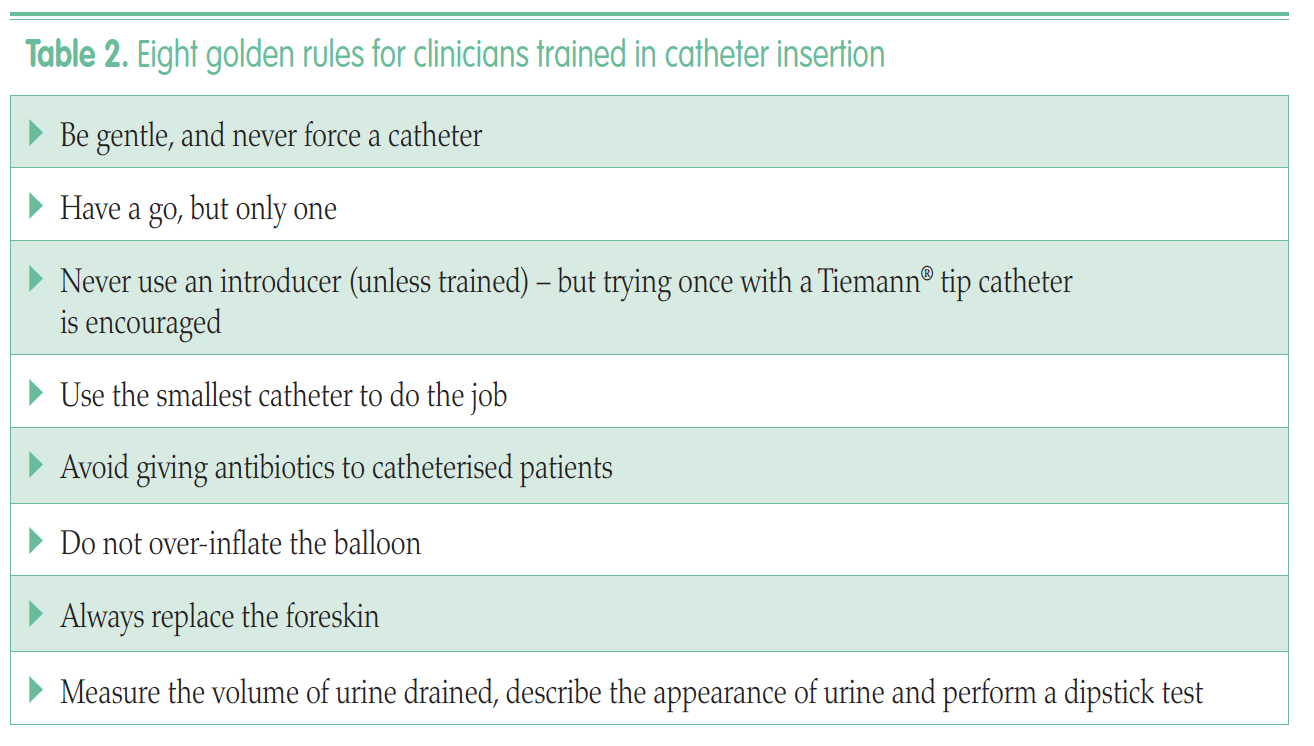
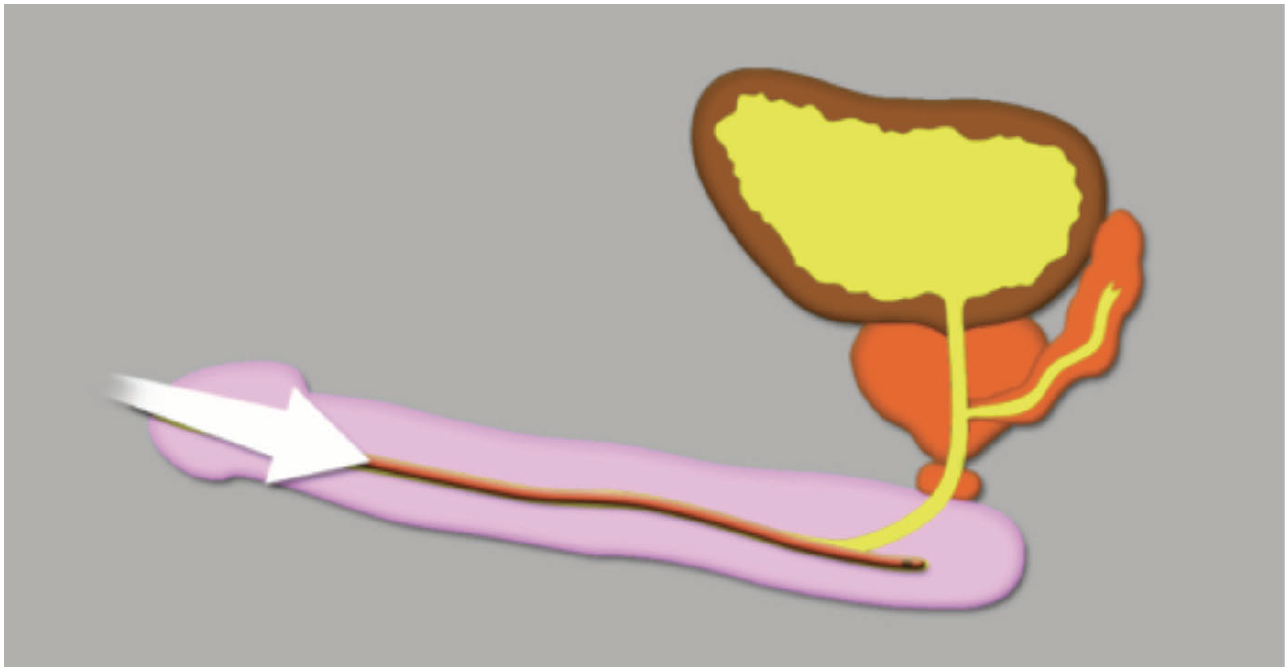 Figure 1.
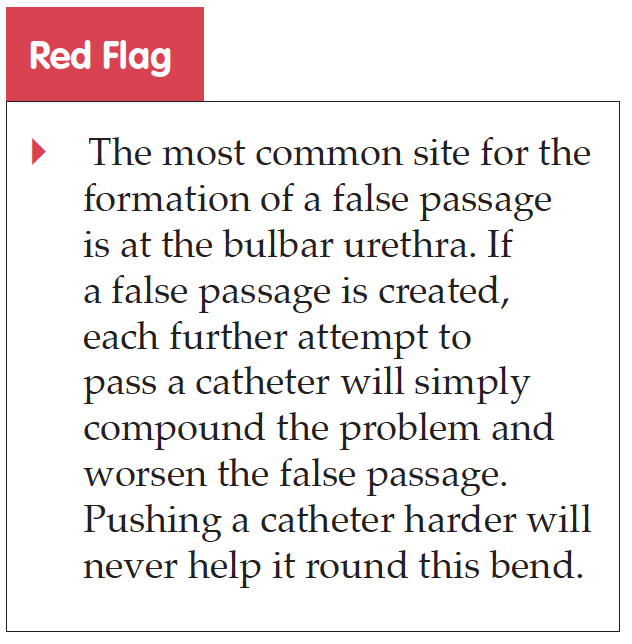
Figure 1.Development of a false passage at the bulbar urethra.
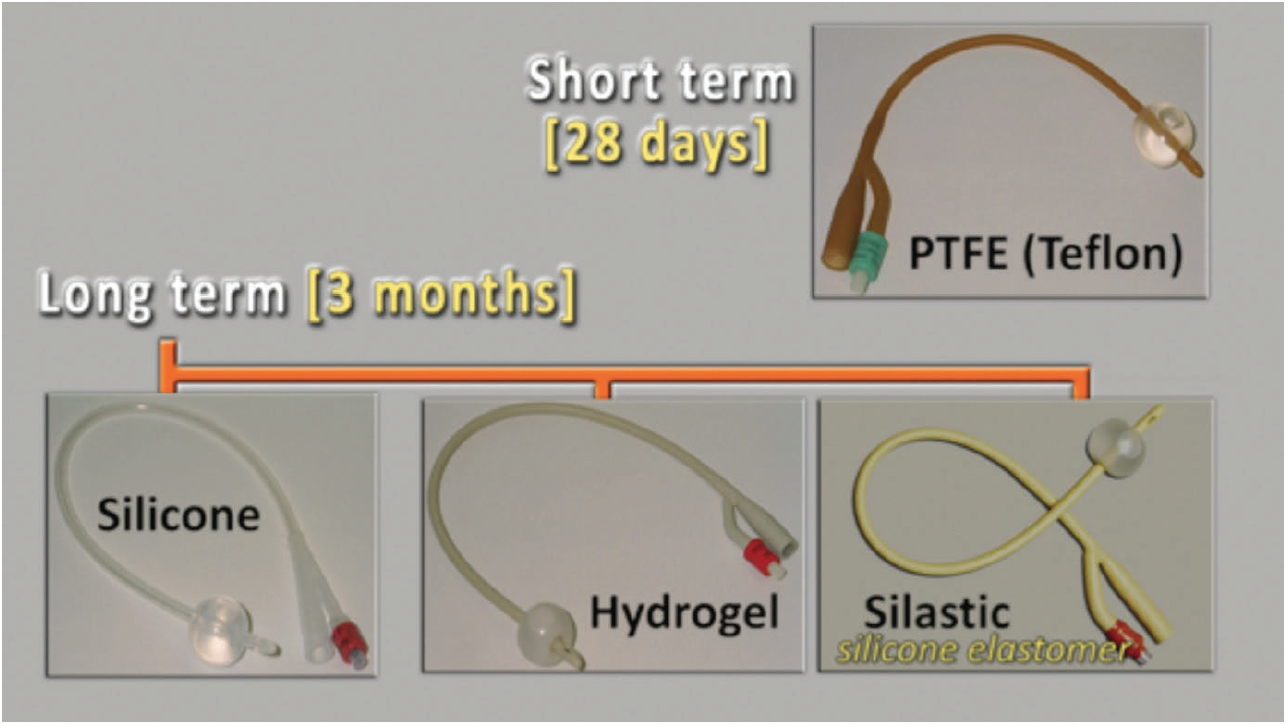 Figure 2.
Figure 2.There are four main types of catheters.
 Figure 3.
Figure 3.Cross-section through a coated latex catheter.
 Figure 4.
Figure 4.Cross-section through an all-silicone catheter.
4. Use the smallest catheter to do the job
 The two natural urethral bends in the male urethra are also the most common sites for urethral strictures to occur, as the catheter may rub resulting in trauma. Trauma within the urethral lumen can result in inflammation. As this heals, there is resultant scar tissue leading to contraction and a tighter, more rigid, passage. This is known as a urethral stricture and markedly reduces the lumen size of the urethra. Therefore, the smallest catheter suitable should always be used, thus minimising disruption to the urethral wall and the risk of future development of urethral strictures.
The two natural urethral bends in the male urethra are also the most common sites for urethral strictures to occur, as the catheter may rub resulting in trauma. Trauma within the urethral lumen can result in inflammation. As this heals, there is resultant scar tissue leading to contraction and a tighter, more rigid, passage. This is known as a urethral stricture and markedly reduces the lumen size of the urethra. Therefore, the smallest catheter suitable should always be used, thus minimising disruption to the urethral wall and the risk of future development of urethral strictures.There are several principles that underpin the concept of an ideal catheter, e.g:
- It should have a good lumen-toexternal diameter ratio to enable maximum drainage
- It should have a low coefficient of friction to minimise trauma to the urethra
- It should be soft and flexible enough not to cause discomfort to the patient and to avoid trauma at pressure points, yet sufficiently strong for the lumen not to be collapsible.
There is only one type of ‘short-term’ catheter, which is constructed from latex coated in polytetrafluoroethylene (PTFE), commonly known as Teflon. With time, degradation of the outer Teflon coating leads to the development of micro-cracks. This catheters should therefore be changed every 28 days.
There are three other commonly used catheter types, which are all considered ‘long-term’ catheters and should be changed every 12 weeks. Hydrogel-coated latex catheters have hydrophilic properties, giving them an exceptionally low coefficient of friction, reducing trauma to the urethra. Secondly, there are silastic catheters, which are made from latex coated in silicone elastomer. These have a hydrophobic surface, which results in a smooth and atraumatic catheter surface. These are the most flexible, but, as a result, have the most collapsible lumen. Finally, there are catheters that are all silicone and so are safe for anyone with a known latex sensitivity. They are less collapsible, but this also renders them to be less flexible. They have a larger drainage lumen when compared to a latex catheter (Figures 3 and 4).
'The two natural urethral bends in the male urethra are also the most common sites for urethral strictures to occur. They are the sites where the catheter may rub the most, resulting in trauma.'
5. Avoid antibiotics in catheterised patients
 Perhaps the biggest controversy that confuses healthcare professionals is the role of antibiotics in catheter care. The presence of a catheter in the human urinary tract effectively creates a dynamic biological ecosystem. When a catheter is inserted, a muco-protein film begins to develop on its surface — produced by the bladder urothelium. At the same time, bacteria ascend along the catheter and start to colonise the urinary system. Within 24 hours, all catheterised bladders are colonised with bacteria. Therefore, any patient who has had a catheter in place for more than one day will have a positive dipstick test of urine to leucocytes and nitrites. This is not infection, but rather normal colonisation due to the presence of a catheter. It is therefore essential to avoid doing a dipstick on urine from an existing catheter. Antibiotics will never eradicate this bacterial fauna, indeed, the exposure of antimicrobials to this ecosystem will simply clone out antibiotic resistance in a system where microbial colonisation is normal and unchangeable. The course, thus provides guidance on how antibiotic administration should be both limited and used effectively. Messages which are in keeping with the teaching of both the World Health Organization (WHO) and Health Education England (HEE, 2015).
Perhaps the biggest controversy that confuses healthcare professionals is the role of antibiotics in catheter care. The presence of a catheter in the human urinary tract effectively creates a dynamic biological ecosystem. When a catheter is inserted, a muco-protein film begins to develop on its surface — produced by the bladder urothelium. At the same time, bacteria ascend along the catheter and start to colonise the urinary system. Within 24 hours, all catheterised bladders are colonised with bacteria. Therefore, any patient who has had a catheter in place for more than one day will have a positive dipstick test of urine to leucocytes and nitrites. This is not infection, but rather normal colonisation due to the presence of a catheter. It is therefore essential to avoid doing a dipstick on urine from an existing catheter. Antibiotics will never eradicate this bacterial fauna, indeed, the exposure of antimicrobials to this ecosystem will simply clone out antibiotic resistance in a system where microbial colonisation is normal and unchangeable. The course, thus provides guidance on how antibiotic administration should be both limited and used effectively. Messages which are in keeping with the teaching of both the World Health Organization (WHO) and Health Education England (HEE, 2015).It is important to remember that when a catheter is draining the bladder, semen from the prostate will also often leak alongside the tube, as there is no other escape for it. A common misconception is that this represents pus, and while it may be, this would be in the context of an acutely unwell patient. Semen often dries out causing an irregular encrustation along the catheter surface. Thus, in an asymptomatic, clinically well male patient, who notices encrusting or fluid around the catheter at the urethral meatus, this does not equate to infection and the need for antibiotics. A suprapubic catheter should be considered for patients with longterm catheters, as it has the benefit of not impeding semen flow.
Constant awareness of the fifth of these golden rules will help to reduce antibiotic resistance and improve clinical practice.
6. Do not overinflate the balloon
Catheter balloons are designed to keep the catheter safely in position, reducing the likelihood of it slipping into the prostate and/or falling out. Usually the balloon is filled to 10ml. Most Foley balloons can manage a volume in excess of 90ml before they burst. However, a larger volume can cause significant trouble for the bladder, as irritation from a catheter balloon can result in detrusor instability, causing bladder spasms and urine bypassing along the outside of the catheter.KEY POINTS
- There are many different catheter-related problems encountered in clinical practice.- Problems with catheters can cause considerable morbidity.
- An educational programme has been developed to improve catheter care across primary and seconday care settings.
- Key areas of catheter care include use of antibiotics, insertion and catheter size.
- Feedback has highlighted new emerging concerns and misconceptions around catheter care.
TAKE-HOME MESSAGE
In the authors’ clinical opinion, there is scope for improvement to reduce controversy and variations in practice around catheter use and management. One programme, the Secret Life of Catheters, has been specifically designed to enhance the care and experience of patients by providing education to improve both the confidence of healthcare professionals and continence care provision.References
Andrews HO, Nauth-Misir R, Shah PJ (1998) Iatrogenic hypospadias — a preventable injury? Spinal Cord 36: 177–80
Ansell T, Harari D (2017) Urinary catheter-related visits to the emergency department and implications for community services. Br J Nurs 26(9): S4–11
Ansell T, Lawton S, Hopper A (2017) Reducing Harm from Urinary Catheters: A Collaborative Approach in South London. Health Innovation Network, London: 1–31
Allegranzi B, Nejad SB, Combescure C et al (2011) Burden of endemic healthcare- associated infection in developing countries: systematic review and metaanalysis. Lancet 377(9761): 228–41
Chapple A, Prinjha S, Feneley R, Ziebland S (2016) Drawing on accounts of longterm urinary catheter use: design for the ‘seemingly mundane’. Qual Health Res 26(2): 154–63
Cottenden A, Bliss D, Buckley B, et al (2013) Management using continence products. In: Abrams P, Cardozo L, Khoury S, Wein A (eds) Incontinence. 5th edn. European Association of Urology and International Consultation on Urological Diseases, Arnhem, The Netherlands: 1651–1786
Ewbank L, Thompson J, McKenna H (2017) NHS hospital bed numbers: past, present future. The King’s Fund, London
Foley FEB (1937) A hemostatic bag catheter. Journal of Urology 38: 137–9
Getliffe KA (1994) The characteristics and management of patients with recurrent blockage of long-term urinary catheters. J Adv Nurs 20(1): 140–49
Getliffe K, Newton T (2006) Catheterassociated urinary tract infection in primary and community health care. Age Ageing 35(5): 477–81
Gage H, Avery M, Flannery C, Williams P, Fader M (2017) Community prevalence of long-term urinary catheters use in England. Neurourol Urodyn 36(2): 293–96
Health Education England (2015) Antimicrobial Stewardship: Start smart - then focus. HEE, London. Available online: https://assets.publishing.service. gov.uk/government/uploads/system/uploads/attachment_data/file/417032/Start_Smart_Then_Focus_FINAL.PDF (accessed January 2019)
Hunter KF, Bharmal A, Moore KN (2013) Long-term bladder drainage: Suprapubic catheter versus other methods: A scoping review. Neurourol Urodyn 32(7): 944–51
Khan AA, Mathur S, Feneley R, Timoney AG (2007) Developing a strategy to reduce the high morbidity of patients with long-term urinary catheters: the BioMed catheter research clinic. BJU Int 100(6): 1298–301
Kohler-Ockmore J, Feneley R (1996) Long-term catheterization of the bladder. Br J Urol International 77(3): 347–51
Kunln CM, Douthitt S, Dancing J, Anderson J, Moeschberger M (1992) The association between the use of urinary catheters and morbidity and mortality among elderly patients in nursing homes. Am J Epidemiol 135(3): 291–301
McNulty C, Freeman E, Smith G, et al (2003) Prevalence of urinary catheterization in UK nursing homes. J Hosp Infect 55(2): 119–23
NHS England (2014) NHS Five Year Forward View. NHS England, Leeds
Saint S, Trautner BW, Fowler KE, Colozzi J, Ratz D, Lescinskas E, Hollingsworth JM, Krein SL (2018) A multicenter study of patient-reported infectious and noninfectious complications associated with indwelling urethral catheters. JAMA Intern Med 178(8): 1078–85
Tay LJ, Lyons H, Karrouze I, et al (2016) Impact of the lack of community urinary catheter care services on the Emergency Department. BJU Int 118(2): 327–34
Wagg A, Potter J, Peel P, Irwin P, Lowe D, Pearson M (2008) National audit of continence care for older people: management of urinary incontinence. Age Ageing 37(1): 39–44
Wilde MH, Brasch J, Getliffe K, et al (2010) Study on the use of long-term urinary catheters in community-dwelling individuals. J Wound Ostomy Continence Nurs 37(3): 301–10
World Health Organization. Antimicrobial Resistance. Available online: www.who.int/antimicrobial-resistance/en/ (last accessed 24 January, 2019)
Ansell T, Harari D (2017) Urinary catheter-related visits to the emergency department and implications for community services. Br J Nurs 26(9): S4–11
Ansell T, Lawton S, Hopper A (2017) Reducing Harm from Urinary Catheters: A Collaborative Approach in South London. Health Innovation Network, London: 1–31
Allegranzi B, Nejad SB, Combescure C et al (2011) Burden of endemic healthcare- associated infection in developing countries: systematic review and metaanalysis. Lancet 377(9761): 228–41
Chapple A, Prinjha S, Feneley R, Ziebland S (2016) Drawing on accounts of longterm urinary catheter use: design for the ‘seemingly mundane’. Qual Health Res 26(2): 154–63
Cottenden A, Bliss D, Buckley B, et al (2013) Management using continence products. In: Abrams P, Cardozo L, Khoury S, Wein A (eds) Incontinence. 5th edn. European Association of Urology and International Consultation on Urological Diseases, Arnhem, The Netherlands: 1651–1786
Ewbank L, Thompson J, McKenna H (2017) NHS hospital bed numbers: past, present future. The King’s Fund, London
Foley FEB (1937) A hemostatic bag catheter. Journal of Urology 38: 137–9
Getliffe KA (1994) The characteristics and management of patients with recurrent blockage of long-term urinary catheters. J Adv Nurs 20(1): 140–49
Getliffe K, Newton T (2006) Catheterassociated urinary tract infection in primary and community health care. Age Ageing 35(5): 477–81
Gage H, Avery M, Flannery C, Williams P, Fader M (2017) Community prevalence of long-term urinary catheters use in England. Neurourol Urodyn 36(2): 293–96
Health Education England (2015) Antimicrobial Stewardship: Start smart - then focus. HEE, London. Available online: https://assets.publishing.service. gov.uk/government/uploads/system/uploads/attachment_data/file/417032/Start_Smart_Then_Focus_FINAL.PDF (accessed January 2019)
Hunter KF, Bharmal A, Moore KN (2013) Long-term bladder drainage: Suprapubic catheter versus other methods: A scoping review. Neurourol Urodyn 32(7): 944–51
Khan AA, Mathur S, Feneley R, Timoney AG (2007) Developing a strategy to reduce the high morbidity of patients with long-term urinary catheters: the BioMed catheter research clinic. BJU Int 100(6): 1298–301
Kohler-Ockmore J, Feneley R (1996) Long-term catheterization of the bladder. Br J Urol International 77(3): 347–51
Kunln CM, Douthitt S, Dancing J, Anderson J, Moeschberger M (1992) The association between the use of urinary catheters and morbidity and mortality among elderly patients in nursing homes. Am J Epidemiol 135(3): 291–301
McNulty C, Freeman E, Smith G, et al (2003) Prevalence of urinary catheterization in UK nursing homes. J Hosp Infect 55(2): 119–23
NHS England (2014) NHS Five Year Forward View. NHS England, Leeds
Saint S, Trautner BW, Fowler KE, Colozzi J, Ratz D, Lescinskas E, Hollingsworth JM, Krein SL (2018) A multicenter study of patient-reported infectious and noninfectious complications associated with indwelling urethral catheters. JAMA Intern Med 178(8): 1078–85
Tay LJ, Lyons H, Karrouze I, et al (2016) Impact of the lack of community urinary catheter care services on the Emergency Department. BJU Int 118(2): 327–34
Wagg A, Potter J, Peel P, Irwin P, Lowe D, Pearson M (2008) National audit of continence care for older people: management of urinary incontinence. Age Ageing 37(1): 39–44
Wilde MH, Brasch J, Getliffe K, et al (2010) Study on the use of long-term urinary catheters in community-dwelling individuals. J Wound Ostomy Continence Nurs 37(3): 301–10
World Health Organization. Antimicrobial Resistance. Available online: www.who.int/antimicrobial-resistance/en/ (last accessed 24 January, 2019)