


Photograph: wavebreakmedia/Shutterstock
PELVIC ORGAN PROLAPSE
Pelvic organ prolapse (POP) has been defined by Haylen et al (2016) as ‘the descent of one or more of the anterior vaginal wall, posterior vaginal wall, the uterus (cervix) or the apex of the vagina (vaginal vault or cuff scar after hysterectomy)’. The most common type of prolapse is found in the anterior vaginal wall (cystocele), then the posterior vaginal wall (rectocele), and finally the uterus or vault (Richardson and Hagen, 2009; Figure 1). Prolapse can occur in isolation but may also co-exist in any combination – many women experience all types of prolapse at once.
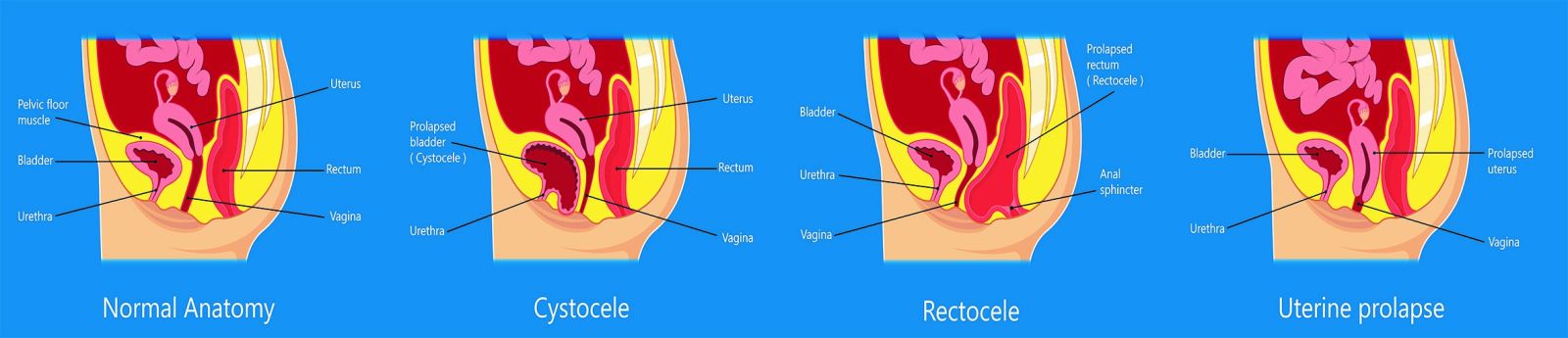
Figure 1. Types of pelvic floor prolapse.
Risk factors
The development of POP is associated with several risk factors (Table 1), most of which the majority of women experience at some point in their lives, making POP such a common problem (Royal College of Obstetricians and Gynaecologists [RCOG], 2013). It is important that the assessor understands these potential risk factors, as if they notice behaviours and patterns which may increase the risk, they are able to highlight them to the patient during assessment and advise accordingly of ways to try and reduce any risk.
Parous women often develop symptoms of POP. Studies suggest that pelvic floor disorders (including POP) are associated with childbirth (Blomquist et al, 2018), because these conditions are often strongly associated with parity. They are more common after vaginal birth than a caesarean section. Observational studies cited by Memon and Landa (2013) have identified that certain methods of delivery appear to be more traumatic to the pelvic floor, particularly forceps delivery, prolonged second stage of labour, and tears to the sphincter. Nulliparous women can, however, also experience symptoms of vaginal prolapse. Someone with symptoms of chronic constipation, for example, may present with symptoms of vaginal prolapse because of the chronic straining and pushing to empty their bowels (Miedel, 2009).
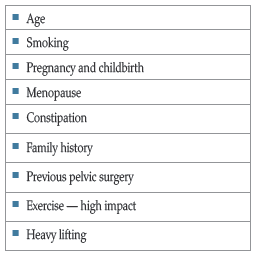
Table 1. Risk factors for developing POP (Vergldt, 2015).
Symptoms
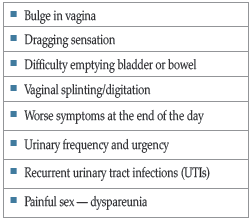
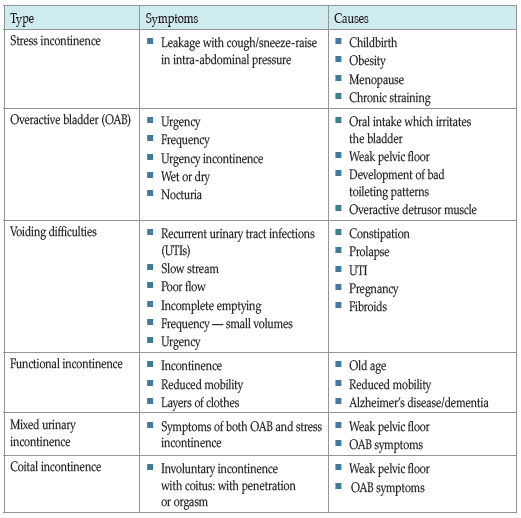
Table 3. Types of urinary incontinence.
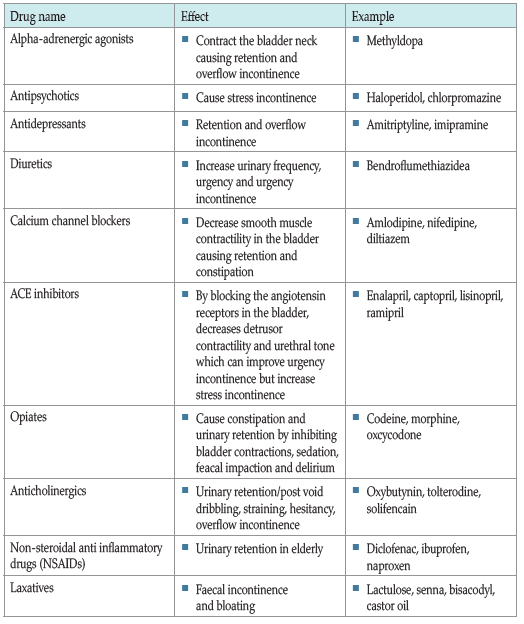
Table 4. Drugs affecting continence (Stewart, 2019).
 RED FLAGS
RED FLAGS
When performing an assessment, it is essential that the assessor is aware of the red flags so that appropriate onward referral can be instigated. These include (National Institute for Health and Care Excellence [NICE], 2019):
- • Microscopic haematuria in women over 50 years
- • Visible haematuria
- • Previous pelvic cancers
- • Persistent bladder or urethral pain
- • Clinically benign pelvic masses
- • Voiding difficulties
- • Suspected urogenital fistula
- • Recurrent UTIs
- • Previous continence surgery
- • Suspected neurological disease
- • Associated faecal incontinence
- • Symptomatic vaginal prolapse
- • Failure of conservative management
- • Complex symptoms.
References
Al-Mali M (2018) Communication skills 3: non-verbal communication. Nurs Times 114(2): 41–2
Bardsley A (2016) An overview of urinary incontinence. Br J Nurs 25(18): S14–S21
Bedoya-Ronga A, Currie I (2014) Improving the management of urinary incontinence. Practitioner 258(1769): 21–4
Blomquist JL, Munoz A, Carroll M, Handa VL, et al (2018) Association of delivery mode with pelvic floor disorders after childbirth. JAMA 320(23): 2438–47
Buckley BS, Lapitan MCM (2010) Prevalence of urinary incontinence in men, women, and children – current evidence: Findings of the Fourth International Consultation on Incontinence. Urology 76(2): 265–70
Boyd C, Stevens D (2020) Urinary incontinence: management in general practice. GM, 20 January 2020. Available online: www.gmjournal.co.uk/urinary-incontinence-in-women-management-in-general-practice
Car J, Choon-Huat Koh G, Sym Foong P, Wang CJ (2020) Video consultations in primary and specialist care during the Covid-19 pandemic and beyond. BMJ 20 Oct: 371:m3945
Colley W (2020) Colley Model. Supporting the assessment of bladder symptoms in adults. Available online: www.continenceassessment.co.uk
Digesu G, Khullar V, Cardozo L, et al (2005) P-QOL: a validated questionnaire to assess the symptoms and quality of life of women with urogenital prolapse. Int Urogynecol J Pelvic Floor Dysfunct 16(3): 176–81; discussion 181
Fedele R (2021) ‘Our eyes became a big way of communicating’: The power of communicating during COVID-19. ANMJ 6 May. Available online: https://anmj.org.au/the-power-of-body-language-in-nursing/
Haylen B, De Ridder D, Freeman R, Swift S, et al (2010) An International Urogynaecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynaecol J 21: 5–26
Haylen BT, Maher CF, Barber MD, Camargo SFM, Dandolu V, Digesu A, et al (2016) International Urogynecological Association (IUGA)/International Continence Society (ICS) Joint Report on the terminology for pelvic organ prolapse (POP). Int Urogynecol J 27(2): 165–94
Herbert J (2009) Pregnancy and childbirth: the effects on pelvic floor muscles. Nurs Times 105(7): 38–41
Laws A (2020) Assessing continence issues during the Covid-19 pandemic. J Community Nurs 34(4): 16–17
Memon H, Landa V (2013) Vaginal childbirth and pelvic floor disorders. Womens Health (Lond) 9(3): 265–77
Miedel A (2009) Non-obstetric risk factors for symptomatic pelvic organ prolapse obstetrics and gynecology. Obstet Gynecol 113(5): 1089–97
Milsom I, Gyhagen M (2019) The prevalence of urinary incontinence. Climacteric 22(3): 217–22
National Institute for Health and Care Excellence (2018) Urinary tract infection (lower): antimicrobial prescribing. NICE, London. Available online: www.nice.org.uk/guidance/ng109
National Institute for Health and Care Excellence (2019) Urinary incontinence and pelvic organ prolapse in women: management. NICE Guideline (NG123) NICE, London
Nazarko L (2015) Person centred care of women with urinary incontinence. Nurse Prescribing 13(6): 288–93
Okamura K, Nojiri Y, Osuga Y (2009) Reliability and validity of the King’s Health Questionnaire for lower urinary tract symptoms in both genders. BJUI 103(12): 1673–78
Pelvic Floor Society (2021) Seizing the opportunity to improve patient care: Pelvic Floor services in 2021 and beyond. Available online: www.pelvicfloorreport.com/wp-content/uploads/2021/04/Pelvic-Floor-Report-V13-WEB.pdf
Rantell A (2017) Assessment and diagnosis of overactive bladder in women. Nurs Standard 27(52): 35–40
Rantell A (2019) Urinary incontinence and pelvic organ prolapse in primary care. Practice Nurs 30(7): 332–37
Richardson K, Hagen S (2009) The role of nurses in the management of women with pelvic organ prolapse. Br J Nurs 18(5): 294-6, 298–300
Royal College of Nursing (online) (2016) Causes of incontinence|Continence|RCN. Available online: www.rcni.com/hosted-content/rcn/continence/causes-of-incontinence
Robinson D, Anders K, Cardozo L, Bidmead J (2007) Outcome measures in urogynaecology: the clinicians’ perspective. Int Urogynecol J Pelvic Floor Dysfunct 18(3): 273–9
Royal College of Nursing (2020) Genital Examination in Women. A resource for skills development and assessment. Available online: www.rcn.org.uk/professional-development/publications/rcn-genital-examination-in-women-pub007961
Royal College of Obstetricians and Gynaecologists (2013) Pelvic organ prolapse. RCOG, London. Available online: www.rcog.org.uk/en/patients/patient-leaflets/pelvic-organ-prolapse/
Stewart E (2019) Urogynaecology. In: Holloway D (2019) Nursing management of Womens Health: a guide for nurse specialists and practitioners. Springer
Vergldt T (2015) Risk factors for pelvic organ prolapse and its recurrence: a systematic review. Int Urogynecolo J 26: 1559–73
Vermeulen CKM, Veen J, Adang C, et al (2021) Pelvic organ prolapse after laparoscopic hysterectomy compared with vaginal hysterectomy: the POP-UP study. Int Urogynecol J 32: 841–50
Wood L, Anger J (2014) Urinary incontinence in women. BMJ Sep 15; 349: g4531
Yates A (2018) How to perform a comprehensive baseline continence assessment. Nurs Times 114(5): 26–9
Yates A (2021) Continence assessment and investigations. J Community Nurs 35(2): 30–7
This article first appeared in the Journal of General Practice Nursing. To cite this article: Stewart E (2021) Pelvic organ prolapse and female urinary incontinence: assessment. J General Practice Nurs 7(4): 54–9