

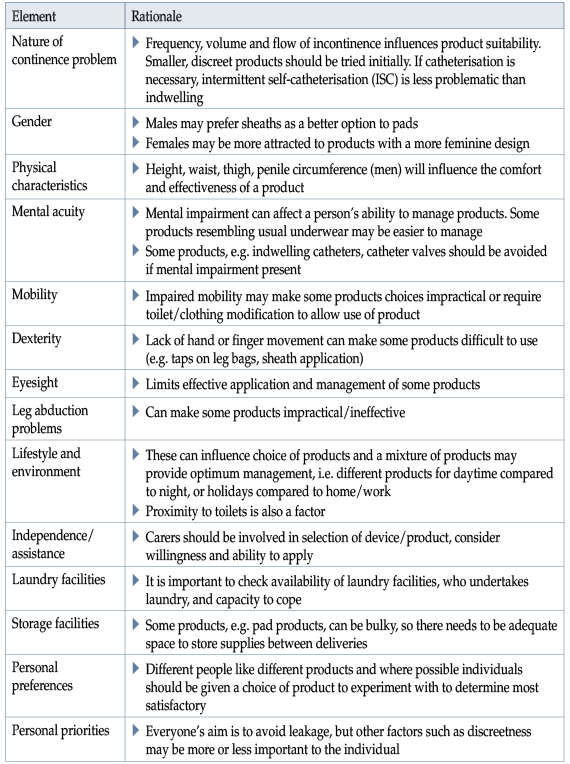
Table 1. Key elements of assessing a patient and their environment for correct management products (ICS, 2017).
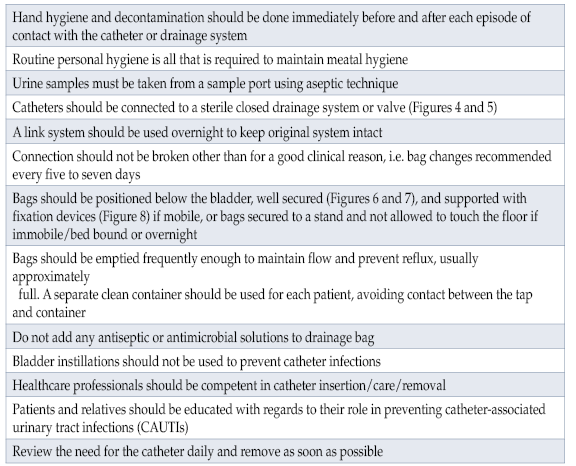
Table 2. Urinary catheter continuing care principles (adapted from Loveday et al, 2014; Yates, 2016; Yates, 2019a).

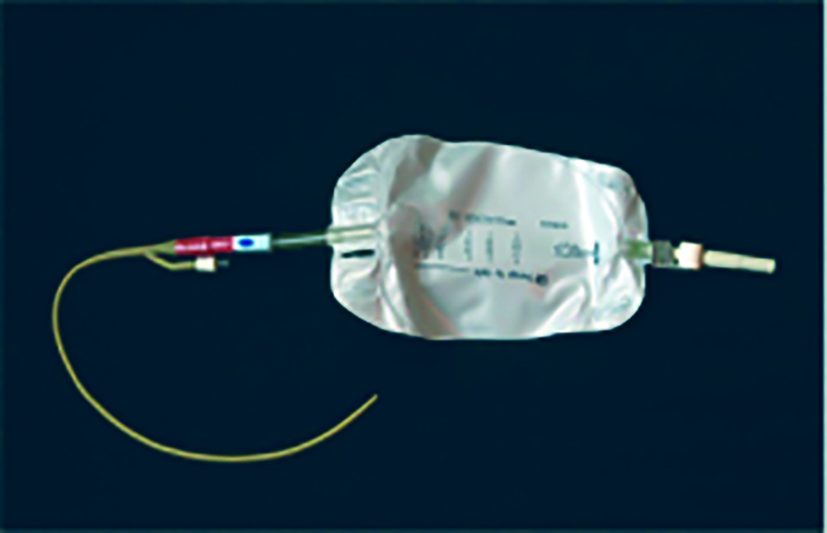
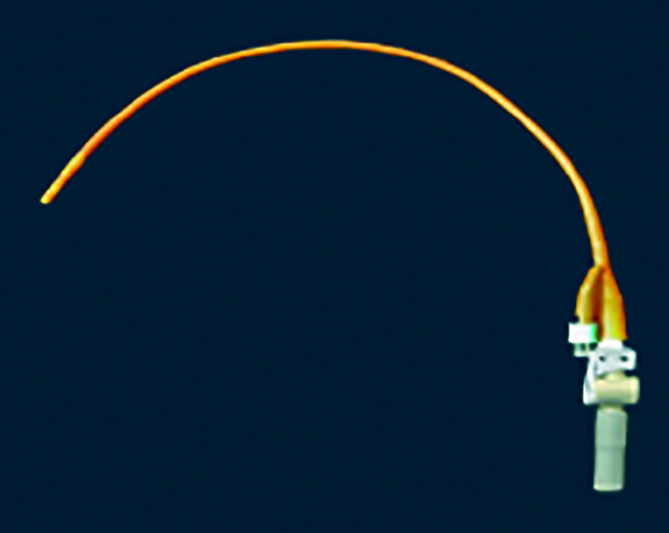

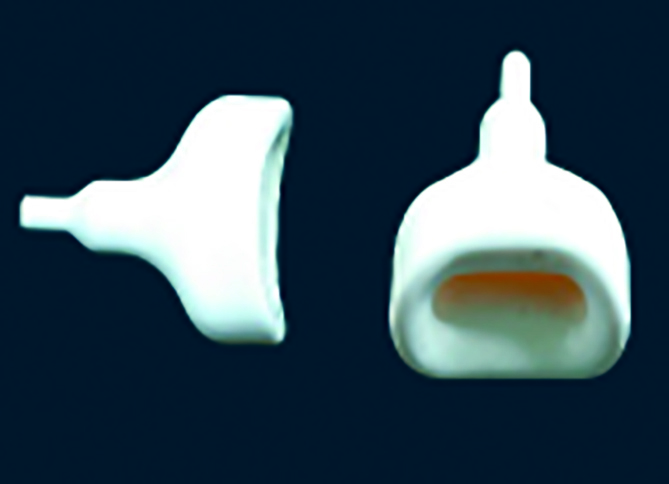

Figure 10. Pocket urinal.
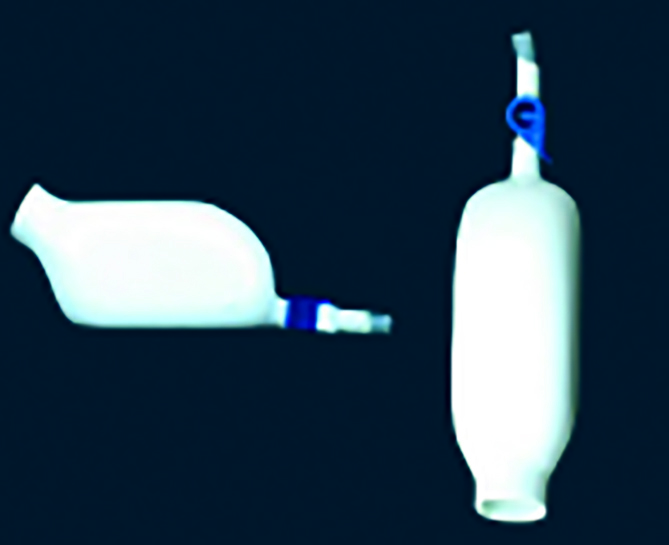

Figure 12. Urine directional aid.
Urinary sheaths
Sheaths, also known as male external catheters (MEC), look in appearance similar to a contraceptive condom (Figure 13). These devices are soft, flexible sleeves designed to fit over the penis and can be attached to a urinary drainage bag or valve. It is vitally important that healthcare professionals are competent in assessing the need for a sheath and have the skill and expertise in applying correctly and passing this knowledge on to individuals (Yates, 2019b). They are available in different materials, sizes, adhesive and non-adhesive, with or without applicators, and have different features such as anti-kinking, anti-blow off to assist drainage (Smart, 2014; Macauley et al, 2015). To use a sheath, individuals should have good dexterity, some degree of penile length, and usually moderate-to-severe urinary incontinence. They may be unsuitable for individuals with confusion, retracted penis, urinary retention or large glans, and narrow penal shaft due to ill fitting (Smart, 2014; ICS, 2017). The main disadvantage of sheaths is that they sometimes fail to stay in place, which is usually due to incorrect sizing or fitting.
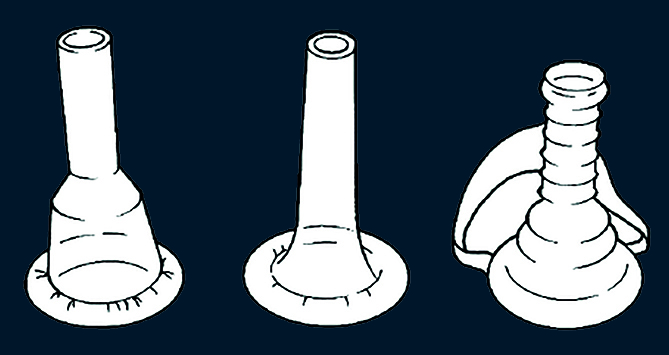
Figure 13. Types of urinary sheaths.
Pubic pressure device
If a sheath is not suitable due to penile retraction, a form of body worn device such as a pubic pressure device may be used (Figure 14). These devices are usually made from latex and require initial assessment and fitting by a specialist.
They are suitable for men (Yates, 2019b):
- With a retracted penis
- With moderate-to-heavy urinary loss
- With urinary urgency/frequency
- Who prefer a body worn device rather than pad products
- With the ability to be mobile/sit in a chair, as they do not work well in a lying position.
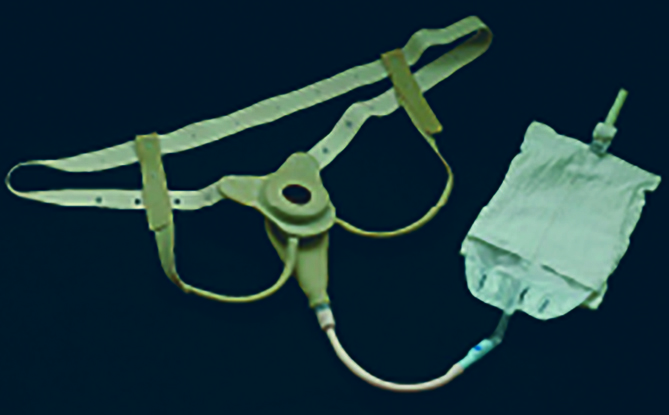
Figure 14. Sample of a pubic pressure device.
EQUIPMENT/DEVICES FOR FAECAL INCONTINENCE
Containing urinary incontinence can be challenging, but faecal incontinence can be extremely difficult to manage and contain. There are certain devices that may assist patients, however, they need to be adequately assessed before use. These include rectal pouches, anal plugs and transanal irrigation (TAI).
Rectal pouches
These are usually adhesive pouches that may be put on to cover the anal canal and collect liquid faeces into the device (Figure 15). They are not suitable for individuals who produce solid faeces or who are mobile. Best results are achieved for immobile bed-bound patients with liquid stool production. There is a risk of skin problems due to adhesive, and especially if the liquid faeces is allowed to be in contact with the skin for some time (ICS, 2017).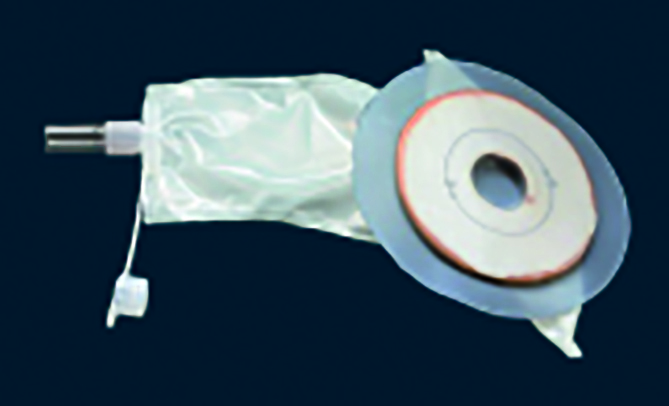
Figure 15. Anal pouch system.Anal plugs
Available in two sizes and on prescription, anal plugs are small devices that can be inserted into the rectum to prevent faecal leakage/seeping. They tend to work better for patients with some degree of lack of rectal sensation, i.e. spina bifida, anorectal malformation, rectal sphincter damage (ICS, 2017), as when inserted and come into contact with bowel mucosa they become like a mushroom (Figure 16), and in patients with complete sensation can trigger the feelings of bowel fullness and frequent expulsion occurs. They can be used on a periodic basis, i.e. special occasions, swimming and when taking exercise.
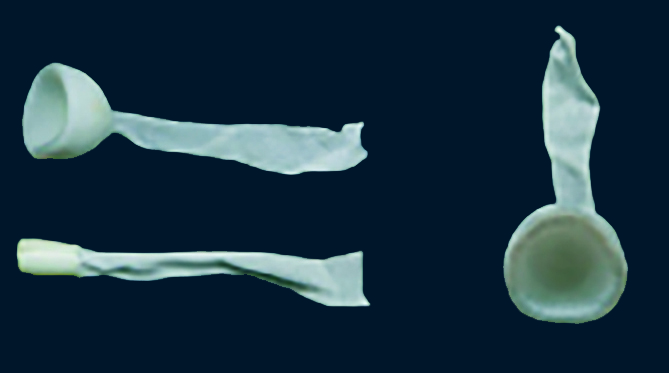
Figure 16. Anal plugs.
Transanal irrigation (TAI)
A developing treatment for faecal incontinence, TAI is designed to empty the rectum and up to the descending colon (according to which device is used). By regularly emptying the bowel in this way, TAI is intended to help re-establish controlled bowel function and enable the user to choose the time, frequency and place of evacuation (Emmanuel et al, 2013; National Institute for Health and Care Excellence [NICE], 2018). In patients who have faecal incontinence, efficient emptying of the distal colon and rectum means that new faeces do not reach the rectum for an average of two days, preventing leakage between irrigations (Henderson et al, 2018; Yates, 2019c).
Before starting TAI, full assessment of the individual should be carried out. TAI has benefits, e.g. it is simple, reversible and minimally invasive, consistent regimen with regular bowel motions, can reduce faecal leakage and individuals can choose time/place of evacuation. However, there are also complications, including worsening of faecal incontinence in some individuals due to the possibility of leakage via irrigation fluid or increased bowel motility (Henderson, 2018; Yates 2019c). Other side-effects or consequences that have been noted are sweating, chills and general discomfort (Henderson et al, 2018; Yates, 2019c).
The device used will vary with what is required by the individual and can range from low volume (Figure 17) to high volume water devices (Figure 18).

Figure 17. Low volume TAI device.

Figure 18. High volume TAI device.
References
Association for Continence Advice (2021) Guidance for the provision of absorbent pad products for adult incontinence. A consensus document. Available online: https://www.aca.uk.com/application/files/8216/2220/2409/Product_Guidance_April_2021.pdf
Carr S (2019) Catheter valves: retraining the bladder to avoid prolonged catheter use. J Community Nurs 33(3): 46–51
Centers for Disease Control and Prevention (2016) National Healthcare Safety Network (NHSN) Overview. Urinary tract infection (catheter-associated urinary tract infection [CAUTI] and non-catheter-associated urinary tract infection [UTI]) and other urinary system infection [USI]) events
Emmanuel AV, Krogh K, Bazzocchi G, et al (2013) Consensus review of best practice of transanal irrigation in adults. Spinal Cord 51(10): 732–8
Fader M, Cottenden A, Chatterton C, et al (2020) An International Continence Society (ICS) report on the terminology for single use body worn absorbent incontinence products. Neurol Urodyn 39: 2031–39
Henderson M,Tinkler L,Yiannakou Y (2018) Transanal irrigation as a treatment for bowel dysfunction. Gastrointestinal Nurs 6(4): 26–34
International Continence Society (2017) Incontinence, 6th edn. Available online: www.ics.org/education/icspublications/icibooks/6thicibook
Lemmens JMH, Broadbridge J, Macaulay M, Rees RW, Archer M, Drake MJ, et al (2019) Tissue response to applied loading using different designs of penile compression clamps. Med Devices 12: 235–43
Loveday H, Wilson JA, Pratt RJ, et al (2014) epic3: National evidence-based guidelines for preventing healthcare-associated infections in NHS hospitals in England. J Hosp Infect 86: S1–70
Macaulay M, Broadbridge J, Gage H, Williams P, Birch B, Moore KN, Cottenden A, Fader M (2015) A trial of devices for urinary incontinence after treatment for prostate cancer. BJU Int 116: 432–42
National Institute for Health and Care Excellence (2018) Peristeen transanal irrigation system for managing bowel dysfunction. Medical technologies guidance MTG36. Available online: www.nice.org.uk/guidance/mtg36
Royal College of Nursing (2021) Catheter Care. RCN Guidance for Professionals. Clinical Professional resource. RCN, London
Simpson P (2017) Long-term urethral catheterisation: guidelines for community nurses. Br J Nurs 26(9 Suppl): S22–S26
Smart C (2014) Male urinary incontinence and the urinary sheath. Br J Nurs 23(9): S20–S25
Soliman Y, Meyer R, Baum MD (2016) Falls in the elderly secondary to urinary symptoms. Rev Urol 18(1): 28–32
Yates A (2016) Indwelling urinary catheterisation: What is best practice? Br J Nurs 25(9): 2–7
Yates A (2017) Urinary catheters 4: teaching intermittent self-catheterisation. Nurs Times 113(4): 49–51
Yates A (2018) Catheter securing and fixation devices: their role in preventing complications. Br J Nurs 27(4): 2–4
Yates A (2019a) Indwelling urinary catheterisation: current best practice. J Community Nurs 32(2): 44–50
Yates A (2019b) Managing male urinary incontinence with sheaths, body worn urinals and penile compression clamps. J Community Nurs 33(5): 40–4
Yates A (2019c) Transanal irrigation: is it the magic intervention for bowel management in individuals with bowel dysfunction? Br J Nurs 29(7): 2–6
This piece was first published in the Journal of Community Nursing. To cite this article use: Yates A (2021) Clinical skills. Part 4: Management with appropriate devices/products. J Community Nurs 35(6): 20-26