

.jpg)
.jpg)
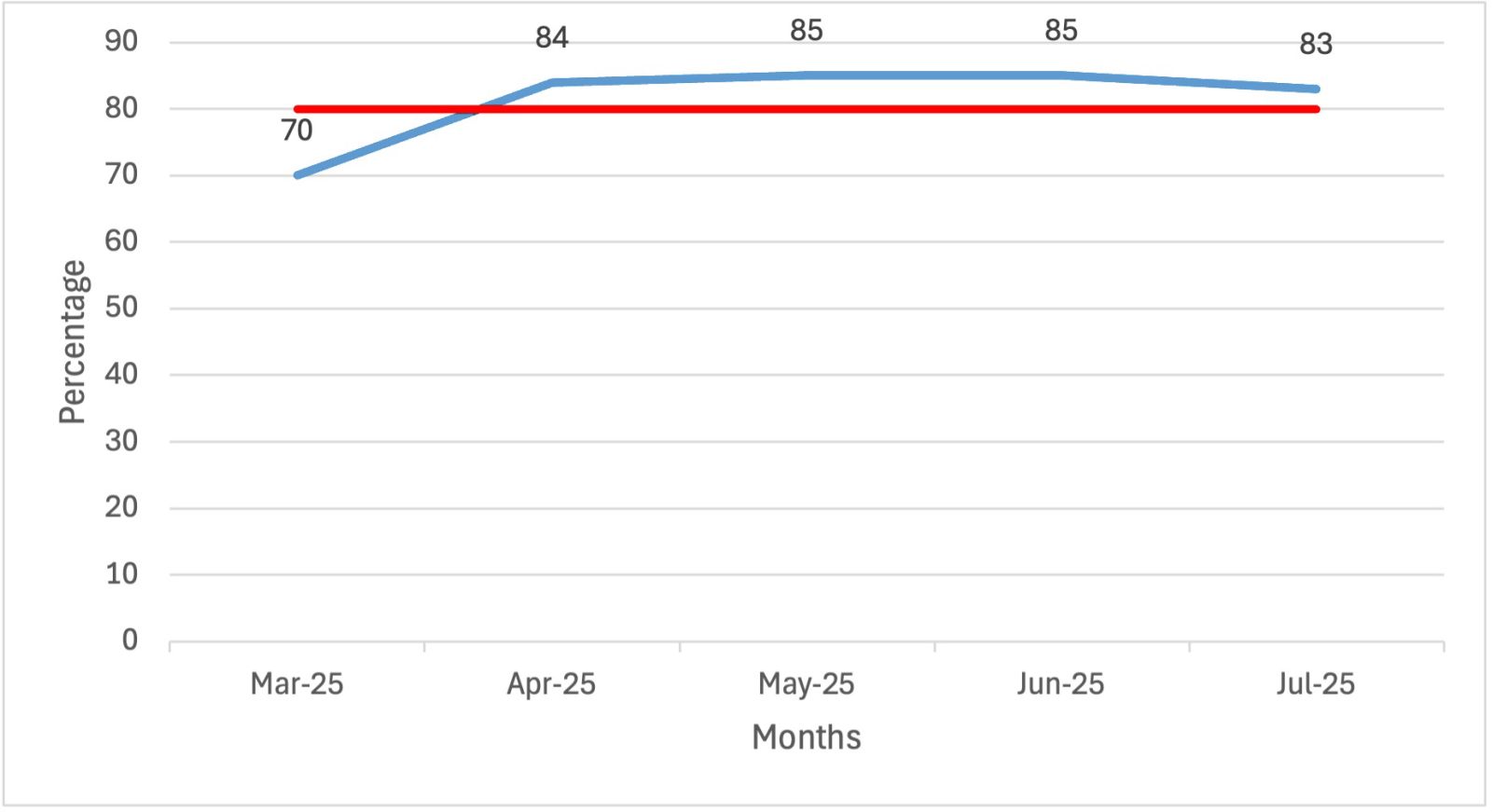
Figure 1. Percentage of patients receiving a diagnosis by 28 days (results of three plan-do-study-act cycles). a. Cycle 1 – on the haematuria pathway. b. Cycle 2 and (c) Cycle 3 – on the straight-to-test pathway.
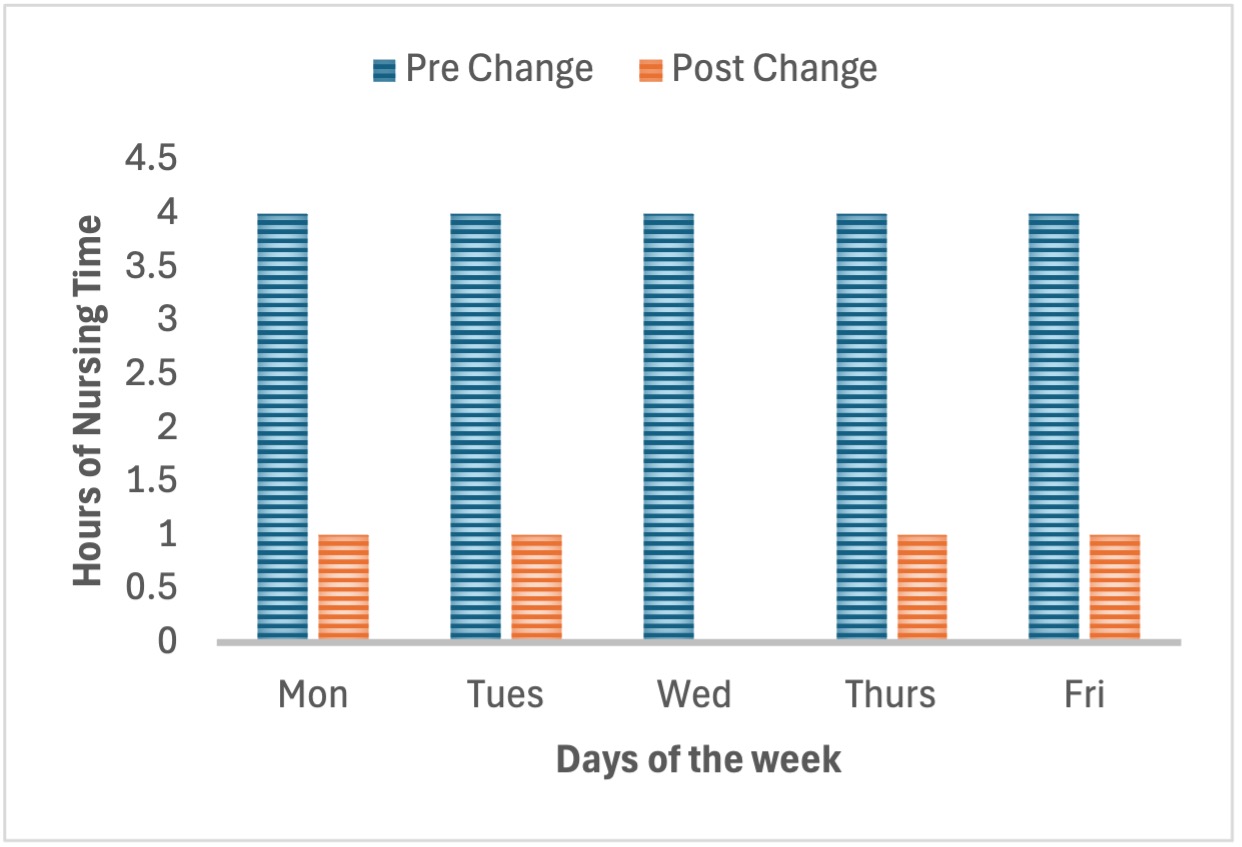
Figure 2. Nursing time spent in clinics.
References
Action Bladder Cancer UK (2025) The facts about bladder cancer. https://actionbladdercanceruk.org/the-facts-about-bladder-cancer/ (accessed 15 September 2025)
British Association of Urological Surgeons (2024) What are the facts about blood in the urine? https://www.baus.org.uk/patients/conditions/2/blood_in_the_urine_haematuria#What_are_the_facts_about_blood_in_the_urine_ (accessed 15 September 2025)
Chew E, Adasonla K, Green J (2023) ‘One-stop’ urgent cancer pathways in urology: What do patients really want? Eur J Surg Oncol. 49(1):e16. https://doi.org/10.1016/j.ejso.2022.11.090
Garrard A, Bashyam A, Pitkin L (2022) Telephone triage for 2-week-wait cancer clinics: a viable alternative to face-to-face clinics? Ann R Coll Surg Engl. 105(4):348-351. https://doi.org/10.1308/rcsann.2022.0103
Getting It Right First Time (2023) Urology: Towards better care for patients with bladder cancer. http://gettingitrightfirsttime.co.uk/wp-content/uploads/2023/09/Urology-Towards-better-care-for-patients-with-bladder-cancer-UPDATED-August-2023.pdf (accessed 15 September 2025)
iRefer (2025) Benefits. https://www.irefer.org.uk/why-irefer/benefits (accessed 15 September 2025)
Jubber I, Shariat SF, Conroy S et al (2020) Non-visible haematuria for the detection of bladder, upper tract, and kidney cancer: an updated systematic review and meta-analysis. Eur Urol. 77(5):583-598. https://doi.org/10.1016/j.eururo.2019.10.010
Macmillan Cancer Support (2025) Causes and risk factors of bladder cancer. https://www.macmillan.org.uk/cancer-information-and-support/bladder-cancer/causes-and-risk-factors-of-bladder-cancer (accessed 15 September 2025)
Macmillan Cancer Support (2025b) Holistic needs assessments. https://www.macmillan.org.uk/healthcare-professionals/innovation-in-cancer-care/holistic-needs-assessment (accessed 15 September 2025)
Meeks JJ (2021) Bladder cancer screening, signs and symptoms, and workup. In: Kamat AM, Black PC, eds. Bladder cancer: a practical guide. Switzerland: Springer Nature
National Institute for Health and Care Excellence (2015) 1.6 Urological cancers. https://www.nice.org.uk/guidance/ng12/chapter/Recommendations-organised-by-site-of-cancer#urological-cancers (accessed 15 September 2025)
NHS England (2019) NHS Long Term Plan ambitions for cancer. https://www.england.nhs.uk/cancer/strategy/ (accessed 15 September 2025)
NHS England (2025a) Faster Diagnosis Framework and the Faster Diagnostic Standard. https://www.england.nhs.uk/cancer/faster-diagnosis/ (accessed 15 September 2025)
NHS England (2025b) Information for service definers. https://digital.nhs.uk/services/e-referral-service/document-library/referral-assessment-services#information-for-service-definers (accessed 15 September 2025)
NHS Health Education England (2022) Case study. Introducing the role of pathway navigator to the South East Region Cancer Alliances - a current project. https://www.skillsforhealth.org.uk/wp-content/uploads/2022/06/ID5-Pathway-Navigator.pdf (accessed 15 September 2025)
Northern Cancer Alliance (2024) Urology. Urgent suspected cancer in adult. https://northerncanceralliance.nhs.uk/wp-content/uploads/2025/05/NCAURO1.pdf (accessed 15 September 2025)
Northern Cancer Alliance (2025) Holistic Needs Assessment (HNA) and Personalised Care and Support Plan (PCSP). https://northerncanceralliance.nhs.uk/pathway/living-with-and-beyond-cancer/recovery-package/holistic-needs-assessment/# (accessed 15 September 2025)
Rai BP, Luis Dominguez Escrig J, Vale L et al (2022) Systematic review of the incidence of and risk factors for urothelial cancers and renal cell carcinoma among patients with haematuria. Eur Urol. 82(2):182-192. https://doi.org/10.1016/j.eururo.2022.03.027
Royal College of Radiologists (2010) Standards for intravascular contrast agent administration to adult patients, Second edition. https://www.bsgar.org/media/BFCR%2810%294_Stand_contrast%283%29.pdf?utm (accessed 15 September 2025)
Wilson RS, Johnston DB, McKay D, Mark D (2022) Straight to test reduces time to investigation and treatment. Ulster Med J. 91(3):139-142
British Association of Urological Surgeons (2024) What are the facts about blood in the urine? https://www.baus.org.uk/patients/conditions/2/blood_in_the_urine_haematuria#What_are_the_facts_about_blood_in_the_urine_ (accessed 15 September 2025)
Chew E, Adasonla K, Green J (2023) ‘One-stop’ urgent cancer pathways in urology: What do patients really want? Eur J Surg Oncol. 49(1):e16. https://doi.org/10.1016/j.ejso.2022.11.090
Garrard A, Bashyam A, Pitkin L (2022) Telephone triage for 2-week-wait cancer clinics: a viable alternative to face-to-face clinics? Ann R Coll Surg Engl. 105(4):348-351. https://doi.org/10.1308/rcsann.2022.0103
Getting It Right First Time (2023) Urology: Towards better care for patients with bladder cancer. http://gettingitrightfirsttime.co.uk/wp-content/uploads/2023/09/Urology-Towards-better-care-for-patients-with-bladder-cancer-UPDATED-August-2023.pdf (accessed 15 September 2025)
iRefer (2025) Benefits. https://www.irefer.org.uk/why-irefer/benefits (accessed 15 September 2025)
Jubber I, Shariat SF, Conroy S et al (2020) Non-visible haematuria for the detection of bladder, upper tract, and kidney cancer: an updated systematic review and meta-analysis. Eur Urol. 77(5):583-598. https://doi.org/10.1016/j.eururo.2019.10.010
Macmillan Cancer Support (2025) Causes and risk factors of bladder cancer. https://www.macmillan.org.uk/cancer-information-and-support/bladder-cancer/causes-and-risk-factors-of-bladder-cancer (accessed 15 September 2025)
Macmillan Cancer Support (2025b) Holistic needs assessments. https://www.macmillan.org.uk/healthcare-professionals/innovation-in-cancer-care/holistic-needs-assessment (accessed 15 September 2025)
Meeks JJ (2021) Bladder cancer screening, signs and symptoms, and workup. In: Kamat AM, Black PC, eds. Bladder cancer: a practical guide. Switzerland: Springer Nature
National Institute for Health and Care Excellence (2015) 1.6 Urological cancers. https://www.nice.org.uk/guidance/ng12/chapter/Recommendations-organised-by-site-of-cancer#urological-cancers (accessed 15 September 2025)
NHS England (2019) NHS Long Term Plan ambitions for cancer. https://www.england.nhs.uk/cancer/strategy/ (accessed 15 September 2025)
NHS England (2025a) Faster Diagnosis Framework and the Faster Diagnostic Standard. https://www.england.nhs.uk/cancer/faster-diagnosis/ (accessed 15 September 2025)
NHS England (2025b) Information for service definers. https://digital.nhs.uk/services/e-referral-service/document-library/referral-assessment-services#information-for-service-definers (accessed 15 September 2025)
NHS Health Education England (2022) Case study. Introducing the role of pathway navigator to the South East Region Cancer Alliances - a current project. https://www.skillsforhealth.org.uk/wp-content/uploads/2022/06/ID5-Pathway-Navigator.pdf (accessed 15 September 2025)
Northern Cancer Alliance (2024) Urology. Urgent suspected cancer in adult. https://northerncanceralliance.nhs.uk/wp-content/uploads/2025/05/NCAURO1.pdf (accessed 15 September 2025)
Northern Cancer Alliance (2025) Holistic Needs Assessment (HNA) and Personalised Care and Support Plan (PCSP). https://northerncanceralliance.nhs.uk/pathway/living-with-and-beyond-cancer/recovery-package/holistic-needs-assessment/# (accessed 15 September 2025)
Rai BP, Luis Dominguez Escrig J, Vale L et al (2022) Systematic review of the incidence of and risk factors for urothelial cancers and renal cell carcinoma among patients with haematuria. Eur Urol. 82(2):182-192. https://doi.org/10.1016/j.eururo.2022.03.027
Royal College of Radiologists (2010) Standards for intravascular contrast agent administration to adult patients, Second edition. https://www.bsgar.org/media/BFCR%2810%294_Stand_contrast%283%29.pdf?utm (accessed 15 September 2025)
Wilson RS, Johnston DB, McKay D, Mark D (2022) Straight to test reduces time to investigation and treatment. Ulster Med J. 91(3):139-142