

A continence service needs to be person-centred and seek to help people identify their needs and agree shared goals. The person experiencing the continence issue should be an active partner in their own care and feel that they have had a good experience (NHS England, 2015). It is important that they are made aware of all the possible options for treatment and be free to choose the approach that will be most likely to meet their individual needs.
The EICC report recommends that as well as treating people with empathy and respect and ensuring that their voice is heard and responded to, a person-centred approach should include person-held records, education about how to manage their condition and prevent a deterioration in their health and, if appropriate, access to personal budgets (NHS England, 2015). People need to experience quick, efficient access to experts who can assess and diagnose the underlying condition or cause of the continence problems and offer effective treatment, self-management and, when required, referral to appropriate specialist services, e.g. urology, urogynaecology, gastroenterology, learning disabilities, neurology, paediatrics, geriatrics, specialist physiotherapy, etc.
True empowerment of people brings choice: not just a choice of provider, but choice of what they feel is appropriate for them. This may mean turning down a particular treatment option. Empowerment means having access to information, advice and treatment and brings the understanding that people have the right to continent living, whenever this is achievable. This enables an optimum quality of life, independence and personal dignity.
 The complexity of continence care is that the root cause is not just one problem, but a myriad of potential and often treatable conditions that span many different specialities (see Mini case examples box). Understanding this complexity and educating health and social care staff (who are most likely to have contact with individuals experiencing continence difficulties) so that they can provide an assessment which gathers the information required for appropriate management or referral pathways is the challenge that health, social and educational institutions need to achieve.
The complexity of continence care is that the root cause is not just one problem, but a myriad of potential and often treatable conditions that span many different specialities (see Mini case examples box). Understanding this complexity and educating health and social care staff (who are most likely to have contact with individuals experiencing continence difficulties) so that they can provide an assessment which gathers the information required for appropriate management or referral pathways is the challenge that health, social and educational institutions need to achieve.
The EICC report recommends that as well as treating people with empathy and respect and ensuring that their voice is heard and responded to, a person-centred approach should include person-held records, education about how to manage their condition and prevent a deterioration in their health and, if appropriate, access to personal budgets (NHS England, 2015). People need to experience quick, efficient access to experts who can assess and diagnose the underlying condition or cause of the continence problems and offer effective treatment, self-management and, when required, referral to appropriate specialist services, e.g. urology, urogynaecology, gastroenterology, learning disabilities, neurology, paediatrics, geriatrics, specialist physiotherapy, etc.
True empowerment of people brings choice: not just a choice of provider, but choice of what they feel is appropriate for them. This may mean turning down a particular treatment option. Empowerment means having access to information, advice and treatment and brings the understanding that people have the right to continent living, whenever this is achievable. This enables an optimum quality of life, independence and personal dignity.
NHS England, 2015
The complexity of continence care is that the root cause is not just one problem, but a myriad of potential and often treatable conditions that span many different specialities (see Mini case examples box). Understanding this complexity and educating health and social care staff (who are most likely to have contact with individuals experiencing continence difficulties) so that they can provide an assessment which gathers the information required for appropriate management or referral pathways is the challenge that health, social and educational institutions need to achieve.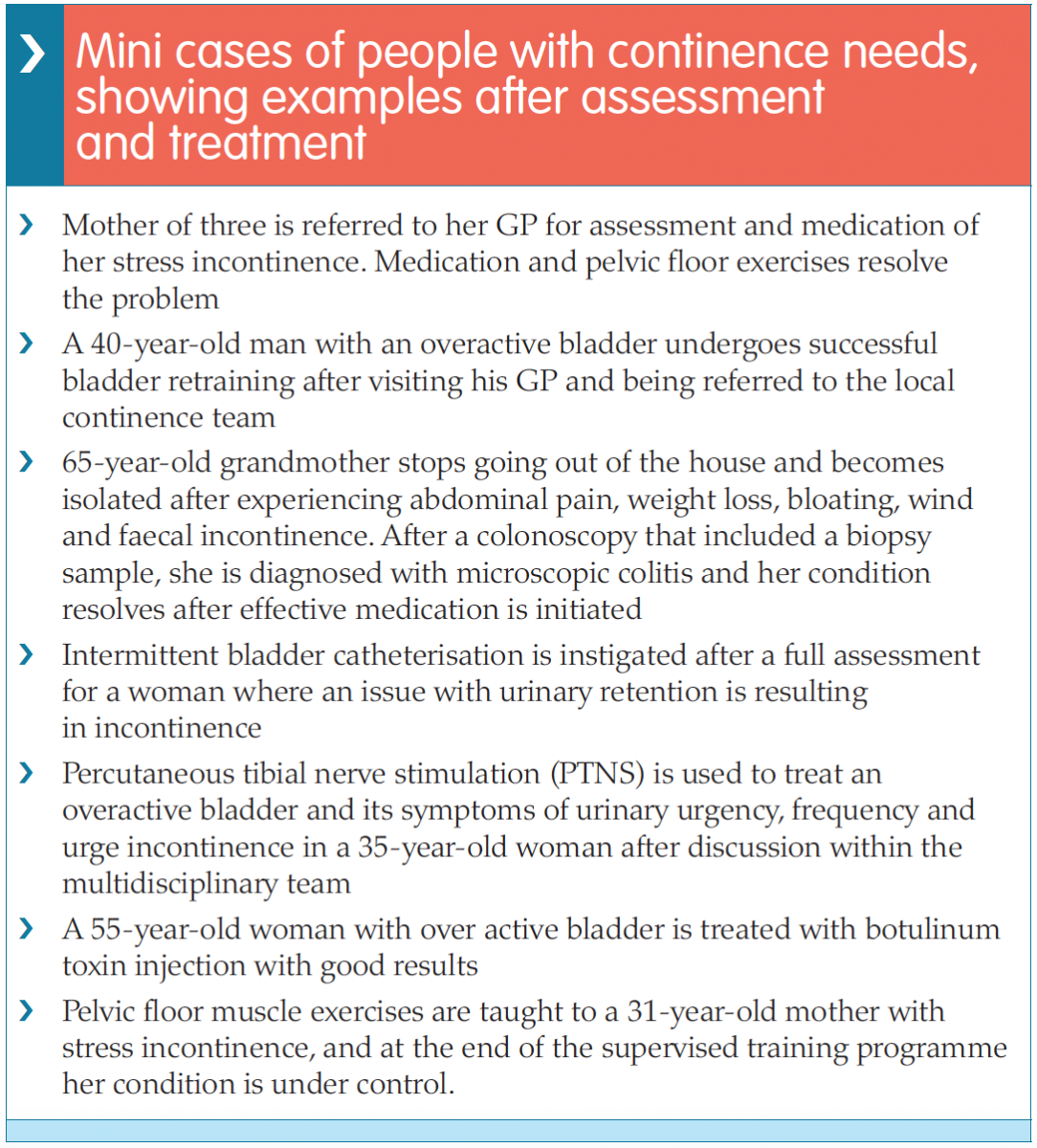
In the UKCS’s guide detailing the minimum standards for continence care, a multidisciplinary team from the UKCS provide modules detailing the knowledge and skills required to provide an effective continence care service across primary, secondary and tertiary settings. These are laid out into eight modules, each providing a simple overview of the learning and minimum standards needed to perform an assessment of, or manage a patient with continence needs:
 The aim of this continence care document is not only to reduce variation in practice across the UK and ensure that all those with continence needs are seen and managed by properly trained staff, but also to improve outcomes in continence care. In addition, the document aims to facilitate the development of appropriate pre and post-registration education by service leads and educational institutions. It is hoped that e-learning packages and study days can be developed using the modules in the guide for healthcare professionals as part of their continuing professional education, and that continence care skills will be included as a mandatory part of pre-registration nurse and other relevant healthcare professional initial training. The UKCC 2015 report recommends that every healthcare professional who encounters patients with continence needs should use the document to identify where their role sits within its framework and take individual responsibility for ensuring that they have the skills and competencies required. This is part of the Nursing and Midwifery Council’s (NMC) requirements for ensuring that nurses have the competencies required to deliver care and can be included as part of reflection and revalidation (NMC, 2015).
The aim of this continence care document is not only to reduce variation in practice across the UK and ensure that all those with continence needs are seen and managed by properly trained staff, but also to improve outcomes in continence care. In addition, the document aims to facilitate the development of appropriate pre and post-registration education by service leads and educational institutions. It is hoped that e-learning packages and study days can be developed using the modules in the guide for healthcare professionals as part of their continuing professional education, and that continence care skills will be included as a mandatory part of pre-registration nurse and other relevant healthcare professional initial training. The UKCC 2015 report recommends that every healthcare professional who encounters patients with continence needs should use the document to identify where their role sits within its framework and take individual responsibility for ensuring that they have the skills and competencies required. This is part of the Nursing and Midwifery Council’s (NMC) requirements for ensuring that nurses have the competencies required to deliver care and can be included as part of reflection and revalidation (NMC, 2015).
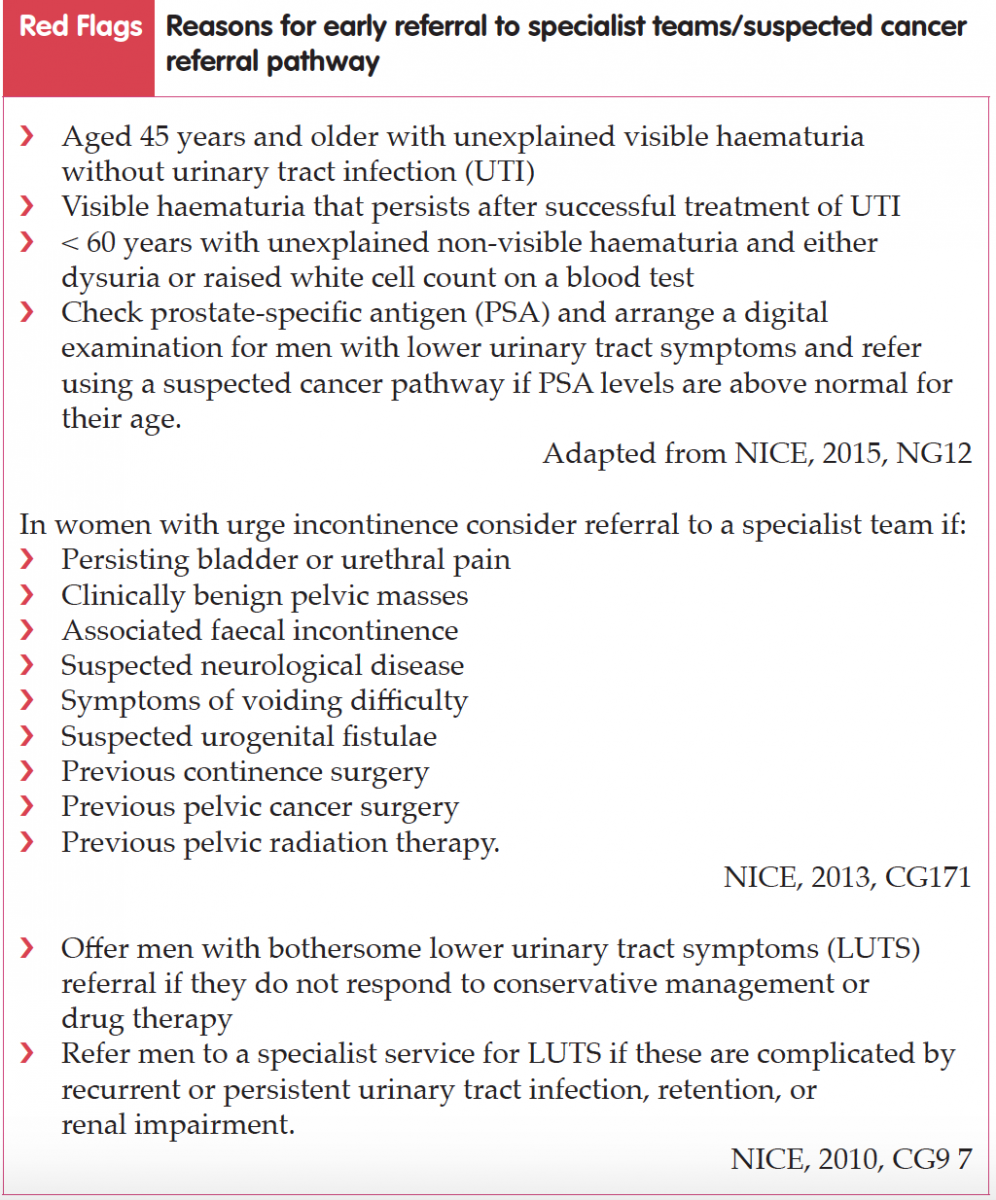
The author, who works as a general practice nurse (GPN), is aware that a number of the patients she sees may have unspoken continence needs. Incontinence is a common problem and the UKCS 2015 report therefore recommends that it should initially be assessed in the community. The basic assessment skills required for this will include having information to give to patients about bladder/bowel function and the use of simple questions to assess this, screening questionnaires, symptom questions, bladder diaries to assess frequency and volume, as well as knowledge on how to refer patients for a bladder scan to assess postvoid residual urine when required. Understanding referral pathways to access specialist care, for example, urodynamic teams, is also important. There is a resource list at the end of this article which will be useful for educating both nurses and patients and explaining the importance of lifestyle intervention, e.g. weight loss, drinking habits as well as pelvic floor exercises, or bladder training. Taking part in an accredited training course is also important. Specialist generalists in the community should be involved with case finding, i.e. asking people the right questions within a routine holistic assessment and providing basic continence care for some, while referring others onto specialist services.
- Module 1: Structure of continence services
- Module 2: Basic assessment and conservative management of bladder and bowel symptoms
- Module 3: Specialist assessment and conservative management of the female lower urinary tract
- Module 4: Specialist assessment and conservative management of the male lower urinary tract (LUT)
- Module 5: Specialist assessment and conservative management of patients with neuropathic bladder
- Module 6: Specialist assessment and conservative management of constipation and faecal incontinence
- Module 7: Urinary catheterisation
- Module 8: Assessment tools.
The aim of this continence care document is not only to reduce variation in practice across the UK and ensure that all those with continence needs are seen and managed by properly trained staff, but also to improve outcomes in continence care. In addition, the document aims to facilitate the development of appropriate pre and post-registration education by service leads and educational institutions. It is hoped that e-learning packages and study days can be developed using the modules in the guide for healthcare professionals as part of their continuing professional education, and that continence care skills will be included as a mandatory part of pre-registration nurse and other relevant healthcare professional initial training. The UKCC 2015 report recommends that every healthcare professional who encounters patients with continence needs should use the document to identify where their role sits within its framework and take individual responsibility for ensuring that they have the skills and competencies required. This is part of the Nursing and Midwifery Council’s (NMC) requirements for ensuring that nurses have the competencies required to deliver care and can be included as part of reflection and revalidation (NMC, 2015).The author, who works as a general practice nurse (GPN), is aware that a number of the patients she sees may have unspoken continence needs. Incontinence is a common problem and the UKCS 2015 report therefore recommends that it should initially be assessed in the community. The basic assessment skills required for this will include having information to give to patients about bladder/bowel function and the use of simple questions to assess this, screening questionnaires, symptom questions, bladder diaries to assess frequency and volume, as well as knowledge on how to refer patients for a bladder scan to assess postvoid residual urine when required. Understanding referral pathways to access specialist care, for example, urodynamic teams, is also important. There is a resource list at the end of this article which will be useful for educating both nurses and patients and explaining the importance of lifestyle intervention, e.g. weight loss, drinking habits as well as pelvic floor exercises, or bladder training. Taking part in an accredited training course is also important. Specialist generalists in the community should be involved with case finding, i.e. asking people the right questions within a routine holistic assessment and providing basic continence care for some, while referring others onto specialist services.
References
British Association of Urological Surgeons Limited (BAUS). Available online: www. baus.org.uk/patients/conditions/5/ incontinence_of_urine (accessed 21 January, 2018)
National Institute for Health and Care Excellence (2010) Lower urinary tract symptoms in men: management (last updated June 2015). Clinical guideline [CG97]. Available online: www.nice.org. uk/guidance/cg97
National Institute for Health and Care Excellence (2013) Urinary incontinence in women: management (last updated November 2015). Clinical guideline [CG171]. Available online: www.nice. org.uk/guidance/cg171
National Institute for Health and Care Excellence (2015) Suspected cancer: recognition and referral (last updated July 2017). NICE guideline [NG12].
Available online: www.nice.org.uk/guidance/ng12 NHS England (2014) Five year forward view. NHS England, London. Available online: www.england.nhs.uk/wpcontent/ uploads/2014/10/5yfv-web.pdf
NHS England (2015) Excellence in continence care: Practical guidance for commissioners, provider, health and social care staff and information for the public. NHS England, London. Available online: www.engalnd.nhs.uk/commisioning/wp-content/uploads/sites/12/2015/11/ EICC-guidance-final-document.pdf
Nursing and Midwifery Council (2015) The Code. NMC, London. Available online: www.nmc.org.uk/globalassets/ sitedocuments/nmc-publications/nmccode.pdf (accessed 22 January, 2018)
United Kingdom Continence Society — continence care steering group (2015) Minimum standards for continence care in the United Kingdom. Available online: www.ukcs.uk.net/wp-content/uploads/2016/04/15091716_Revised_ Min_Standards_for_CC_in_UK.pdf (accessed 21 January, 2018)
National Institute for Health and Care Excellence (2010) Lower urinary tract symptoms in men: management (last updated June 2015). Clinical guideline [CG97]. Available online: www.nice.org. uk/guidance/cg97
National Institute for Health and Care Excellence (2013) Urinary incontinence in women: management (last updated November 2015). Clinical guideline [CG171]. Available online: www.nice. org.uk/guidance/cg171
National Institute for Health and Care Excellence (2015) Suspected cancer: recognition and referral (last updated July 2017). NICE guideline [NG12].
Available online: www.nice.org.uk/guidance/ng12 NHS England (2014) Five year forward view. NHS England, London. Available online: www.england.nhs.uk/wpcontent/ uploads/2014/10/5yfv-web.pdf
NHS England (2015) Excellence in continence care: Practical guidance for commissioners, provider, health and social care staff and information for the public. NHS England, London. Available online: www.engalnd.nhs.uk/commisioning/wp-content/uploads/sites/12/2015/11/ EICC-guidance-final-document.pdf
Nursing and Midwifery Council (2015) The Code. NMC, London. Available online: www.nmc.org.uk/globalassets/ sitedocuments/nmc-publications/nmccode.pdf (accessed 22 January, 2018)
United Kingdom Continence Society — continence care steering group (2015) Minimum standards for continence care in the United Kingdom. Available online: www.ukcs.uk.net/wp-content/uploads/2016/04/15091716_Revised_ Min_Standards_for_CC_in_UK.pdf (accessed 21 January, 2018)