

Over the last few decades, the use of intermittent self-catheterisation (ISC) to control or assist voiding has become widespread. Increasingly, more treatments, both medical and surgical, are possible because of ISC. Alongside this increase in use has been the development and evolution of intermittent catheters themselves. There are also a number of National Institute for Health and Care Excellence (NICE) guidelines advocating the use of ISC (Table 3). Of course, there will always be patients who cannot or will not perform ISC on themselves, either because of physical, practical or psychological impediments; however, it is equally true that not all patients who could benefit from using ISC are necessarily being offered it (Dingwall and McLafferty, 2006).
Lapides et al first published their findings on ISC in 1972, which showed that the procedure was associated with less urinary tract infections (UTIs) than indwelling catheterisation, and that it greatly improved the quality of life of patients with bladder problems. This 1972 paper and subsequent publications by Lapides et al (1974, 1976) and Diokno et al (1983) outlined the main advantages of ISC, which included:
Although not all patients are suitable for ISC, it is increasingly becoming an option, either as treatment or as a consequence of having surgery (Van Achterburg et al, 2007).
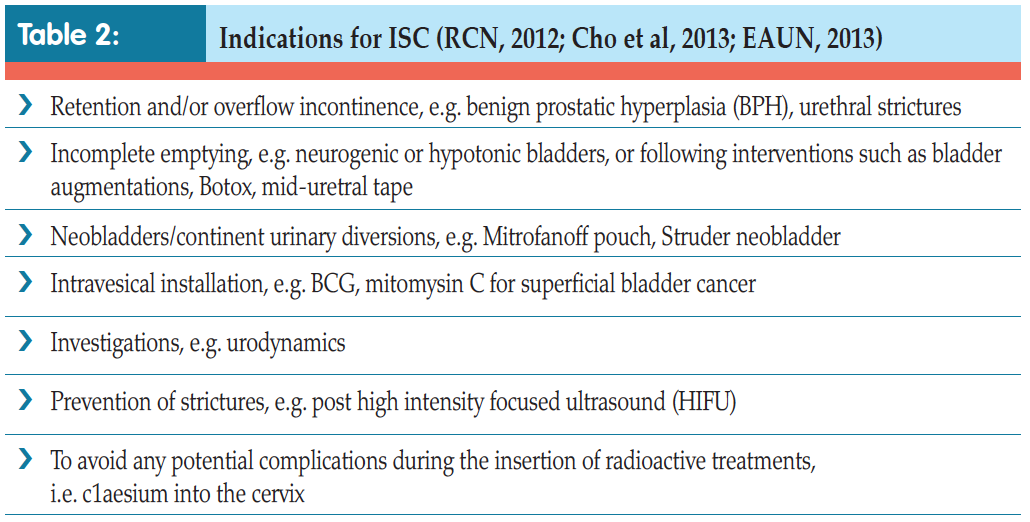
ISC is used to manage voiding for individuals with various problems, including those who, historically, were routinely managed with indwelling catheters for benign prostatic hyperplasia (BPH) or urethral strictures. Incomplete emptying, i.e. in neurogenic or hypotonic bladders, can also be successfully managed with ISC, as can that caused by surgical intervention such as Botox treatment for overactive bladders or following insertion of mid-urethral tape for urinary incontinence. Indeed, many surgical procedures which have become standard nowadays would not be possible without ISC. Continent urinary diversions, such as neobladders, enterocystoplasties, or urinary pouches, e.g. the Mitrofanoff, all rely on the patient being able to successfully self-catheterise to void (European Association of Urology Nurses [EAUN], 2013).
Other indications for the use of ISC include bladder or urethral investigations and intravesical instillation of drugs directly into the bladder, such as Bacillus Calmette– Guérin (BCG) vaccine or mitomycin for superficial bladder cancer (Bohle et al, 2003), or capsaisin for bladder overactivity (Kim and Chancellor, 2000).
It is also not suitable for accurate urine output monitoring, continuous bladder irrigation and immediately following surgery to the lower urinary tract, or where continuous drainage is required in high pressure bladders to avoid kidney damage (EAUN, 2013).
The principles governing ISC are the same as those for indwelling catheters in terms of how to do the procedure safely and to minimise risk to the patient. The main difference is that instead of the healthcare professional catheterising the patient aseptically, it is the patient who learns how to insert the catheter and drain the bladder using a clean rather than aseptic technique.
Research has shown that when done correctly, ISC is a safe procedure which avoids the problems associated with long-term indwelling catheters (Lapides et al, 1972; Igawa et al, 2008). Patients with indwelling catheters are at risk of UTIs, encrustation, stone formation, bladder spasm, urine bypassing and consequent urine leakage and catheter blockage (Feneley et al, 2015). These problems arise because the catheter, which is a foreign body, is usually left in the bladder for long periods of time (4–12 weeks). With ISC, the dwell time in the bladder is only a matter of minutes until all the urine has been drained away, after which the catheter is removed and discarded. This results in less risk of infection and all the consequent problems associated with it. Another advantage is that the patient does not need a permanently placed appliance, or have to deal with an external urine drainage bag, thus reducing the impact of catheterisation on quality of life and allowing the patient to be in control (Igawa et al, 2008; RCN, 2012; EAUN, 2015).
Lapides et al first published their findings on ISC in 1972, which showed that the procedure was associated with less urinary tract infections (UTIs) than indwelling catheterisation, and that it greatly improved the quality of life of patients with bladder problems. This 1972 paper and subsequent publications by Lapides et al (1974, 1976) and Diokno et al (1983) outlined the main advantages of ISC, which included:
- Preventing or overcoming infection by regular emptying of the bladder
- No real increased infection rate using a clean rather than a sterile procedure
- Promoting a ‘normal’ pattern of filling and emptying stages of micturition
- Protecting the upper urinary tract
- Improving symptoms
- Promoting independence
- Improving quality of life.
INTERMITTENT CATHETERISATION
Indications
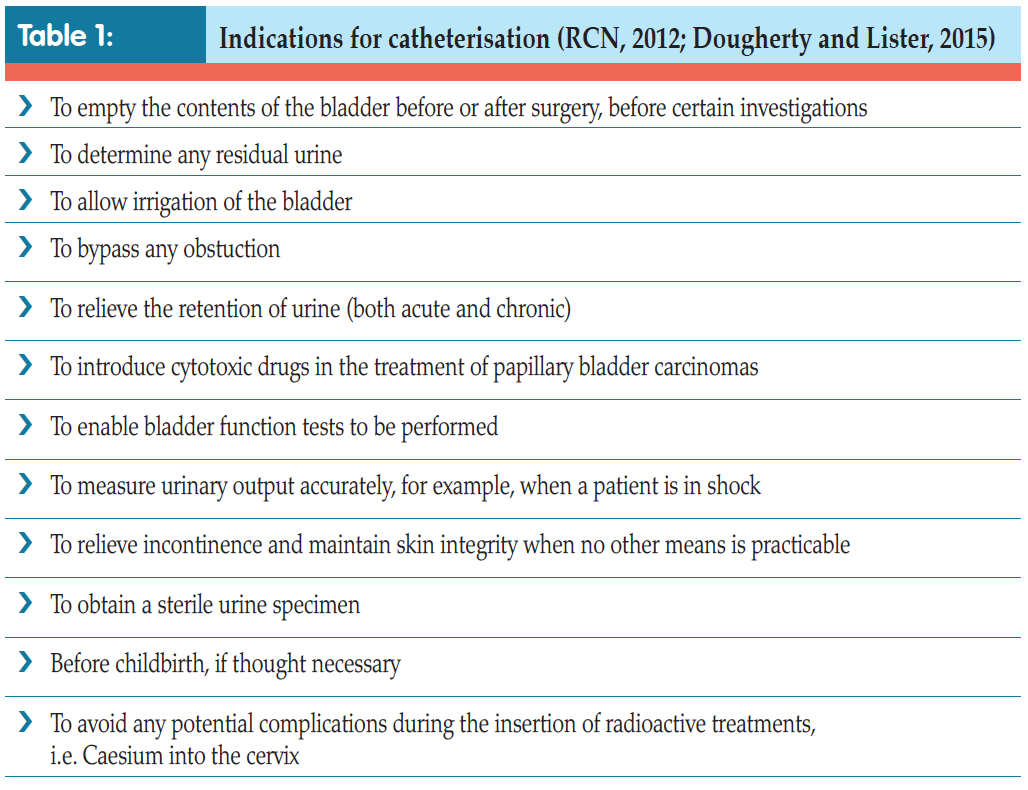
There are several indications for using catheters — both indwelling (see pp. 28–34) and intermittent (Tables 1 and 2).Although not all patients are suitable for ISC, it is increasingly becoming an option, either as treatment or as a consequence of having surgery (Van Achterburg et al, 2007).
ISC is used to manage voiding for individuals with various problems, including those who, historically, were routinely managed with indwelling catheters for benign prostatic hyperplasia (BPH) or urethral strictures. Incomplete emptying, i.e. in neurogenic or hypotonic bladders, can also be successfully managed with ISC, as can that caused by surgical intervention such as Botox treatment for overactive bladders or following insertion of mid-urethral tape for urinary incontinence. Indeed, many surgical procedures which have become standard nowadays would not be possible without ISC. Continent urinary diversions, such as neobladders, enterocystoplasties, or urinary pouches, e.g. the Mitrofanoff, all rely on the patient being able to successfully self-catheterise to void (European Association of Urology Nurses [EAUN], 2013).
Other indications for the use of ISC include bladder or urethral investigations and intravesical instillation of drugs directly into the bladder, such as Bacillus Calmette– Guérin (BCG) vaccine or mitomycin for superficial bladder cancer (Bohle et al, 2003), or capsaisin for bladder overactivity (Kim and Chancellor, 2000).
Contraindications and precautions
ISC is contraindicated in patients with a false passage down the urethra, those who have had trauma to the penis, or have a tumour or other injury. It should be used with caution following prostatic or urethral and bladder surgery, in patients with urethral stents or artificial prosthesis, or those with a tendency to bleed (Royal College of Nursing [RCN], 2012).It is also not suitable for accurate urine output monitoring, continuous bladder irrigation and immediately following surgery to the lower urinary tract, or where continuous drainage is required in high pressure bladders to avoid kidney damage (EAUN, 2013).
 ISC versus indwelling catheters
ISC versus indwelling catheters
The principles governing ISC are the same as those for indwelling catheters in terms of how to do the procedure safely and to minimise risk to the patient. The main difference is that instead of the healthcare professional catheterising the patient aseptically, it is the patient who learns how to insert the catheter and drain the bladder using a clean rather than aseptic technique.Research has shown that when done correctly, ISC is a safe procedure which avoids the problems associated with long-term indwelling catheters (Lapides et al, 1972; Igawa et al, 2008). Patients with indwelling catheters are at risk of UTIs, encrustation, stone formation, bladder spasm, urine bypassing and consequent urine leakage and catheter blockage (Feneley et al, 2015). These problems arise because the catheter, which is a foreign body, is usually left in the bladder for long periods of time (4–12 weeks). With ISC, the dwell time in the bladder is only a matter of minutes until all the urine has been drained away, after which the catheter is removed and discarded. This results in less risk of infection and all the consequent problems associated with it. Another advantage is that the patient does not need a permanently placed appliance, or have to deal with an external urine drainage bag, thus reducing the impact of catheterisation on quality of life and allowing the patient to be in control (Igawa et al, 2008; RCN, 2012; EAUN, 2015).
Not surprisingly, patients found learning ISC daunting, and that it caused them fear, anxiety and embarrassment. Ideally, they wanted to be taught the skill in their home environment. The nurse’s attitude and communication skills were also important in creating a relaxed atmosphere to help alleviate embarrassment and anxiety and enable patients to retain information (Logan et al, 2008; Shaw et al, 2008). The key to keeping patients motivated is having healthcare professionals who are experienced and aware that patients need time and understanding, as well as a proper assessment of their condition and physical and cognitive abilities.
 Thus, teaching ISC should be tailored to each individual. As said, the amount of time it will take to learn and be confident varies from person to person. However, some healthcare professionals have limited time and resources and may not be able to cater to individual needs (Logan, 2017). Unfortunately, this means that patients either get minimum teaching before being expected to start the procedure, or are not followed up once they do so. Patients may be rationed to one face-to-face slot for a scheduled amount of time (e.g. 15–30 minutes), and then followed up by phone. Teaching aids, such as DVDs, sent to patients ahead of appointments can help them to focus on learning the actual technique and so get the greatest benefit from their appointment with the healthcare professional (Logan, 2017).
Thus, teaching ISC should be tailored to each individual. As said, the amount of time it will take to learn and be confident varies from person to person. However, some healthcare professionals have limited time and resources and may not be able to cater to individual needs (Logan, 2017). Unfortunately, this means that patients either get minimum teaching before being expected to start the procedure, or are not followed up once they do so. Patients may be rationed to one face-to-face slot for a scheduled amount of time (e.g. 15–30 minutes), and then followed up by phone. Teaching aids, such as DVDs, sent to patients ahead of appointments can help them to focus on learning the actual technique and so get the greatest benefit from their appointment with the healthcare professional (Logan, 2017).Ideally, patients should be seen as often as they need until they are confident and competent.
 Follow-up
Follow-up
Patients should always be followed up for a period of time. Indeed, time spent with patients at this stage means that they are more likely to comply with care and carry on with ISC (Logan et al, 2008). Adherence to treatment regimens has been found to be directly linked to the patient’s ability to actively accept the need for ISC by establishing early coping strategies, rather than being in denial and avoiding the topic (Shaw and Logan, 2013). Shaw and Logan (2013) also found that reinforcing the positives of ISC and highlighting how it will enable independence and control over bladder function helps patients to achieve a return of some sense of normality, helping them to maintain the integrity of their:
- Self-image
- Privacy
- Dignity
- Self-esteem
- Quality of life.
Currently, all intermittent catheters are single-use only. If inserting the catheter is difficult, patients should be advised to try a different type. Different brands of catheter may feel softer and more
'... patients may need the self-lubricating catheters attached to bags by day to ensure that they can empty their bladder wherever they are, for example, if there is no disabled toilet they can access, but then use ones without a bag when at home.'
pliable or stiffer than others, despite being the same Charrière size. Catheters may also have different shaped tips, such as a tapered or olive tip, while some patients may require a catheter with a curved tip rather than a straight one (a Tiemann or Coude tip catheter). These can be useful if catheterisation is difficult, such as when trying to get past an enlarged prostate.
There are also catheters which are already attached to a urine drainage bag. This is especially useful when not in the vicinity of a toilet, or if the patient is in a wheelchair or cannot transfer onto the toilet for whatever reason. Here, urine drains directly into the bag and then can be disposed of later (EAUN, 2013).
A mixture of catheters can be used to suit different aspects of daily life. For example, patients may need the self-lubricating catheters attached to bags by day to ensure that they can empty their bladder wherever they are, for example, if there is no disabled toilet they can access, but then use ones without a bag when at home. There are also different aids available to help with dexterity or positioning issues (Figure 1).

Figure 1. Aids to hold catheter in place or to allow a better grip.
Bleeding
It is also important to reassure patients that some slight bleeding when the urine starts to drain, or some blood on the catheter tip when it is withdrawn, are normal, although prolonged and heavy bleeding is not (RCN, 2012). If this happens, they should seek help (Bardsley, 2015).
Leaking urine in between catheterisations
Some patients may still leak urine in-between catheterisations and again this may impact on their adhering to the treatment regimen. Asking the patient to keep a threeday diary of all their fluid input and urine output and indicating when they leak will give a picture of how often they are doing the procedure and if they are emptying the bladder properly. Again, they may need their technique reassessed to ensure that they are emptying properly and completely. It might mean that patients need to increase the number of times they catheterise during the day and adjust how much fluid, and when they drink it, during the day, to have longer dry spells. Once again, anticholinergic medication may help if the bladder is overactive and the leak is a result of bladder spasms (Barton, 2010; Mangnall, 2012).
Other complications
Other problems on immediate catheterisation include formation of a false passage and very rarely bladder perforation (especially in reconstructed bladders, such as neobladders or enterocystoplasties) and urethral strictures. There is still the possibility of chronic bacteriuria, although this is less so than with indwelling catheters. Other issues that might arise include epididymitis, urethritis and prostatitis. Patients can also produce bladder stones. This is rare, but can happen especially if the patient has a reconstructed bladder made of bowel and so has a lot of mucus sitting in the bladder, which is not drained out and/or washed out regularly (EAUN, 2013). Table 3 outlines NICE guidelines which advocate use of ISC in bladder care of certain patient groups.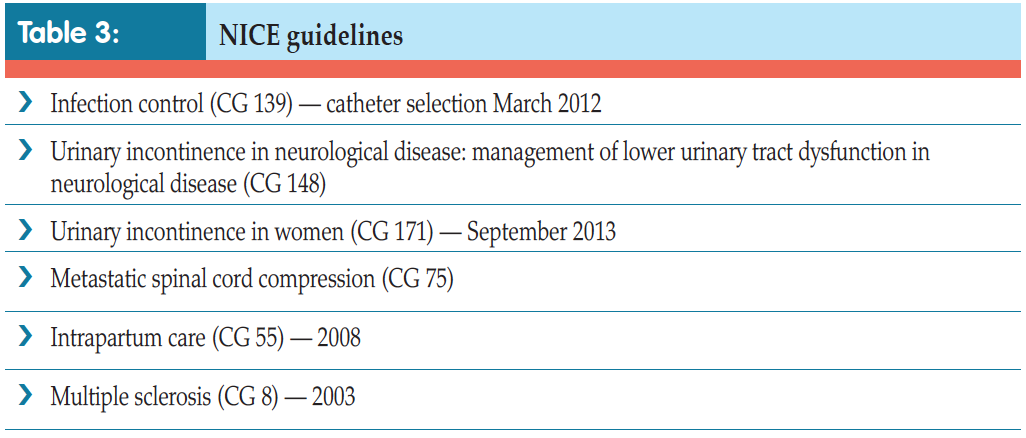
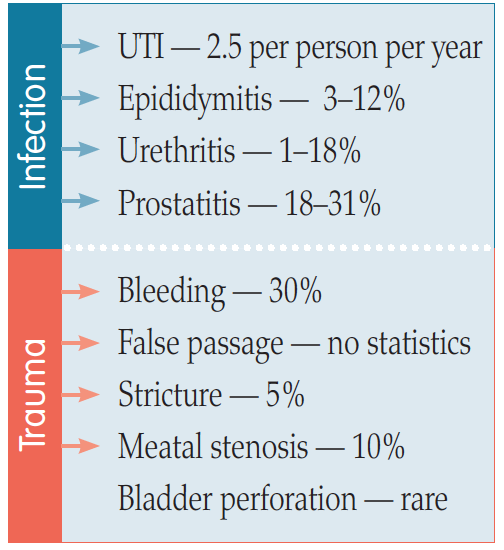
Figure 2. Complications of ISC (EAUN, 2013).
References
Addison R, Foxley S, Mould W, et al (2012) Catheter care RCN guidance for nurses. RCN, London. Available online: http:// studyres.com/doc/8027570/cathetercare- rcn-guidance-for-nurses?page=2
Bardsley A (2015) ISC in women following urogynaecologic surgery. Br J Nurs (urology supplement) 20(18): S6–S13
Barton R (2000) Intermittent self catheterisation. Nurs Standard 15(9): 47–52
Bohle A, Jocham D, Bock PR (2003) Intravesical bacillus Calmette-Guerin versus mitomycin C for superficial bladder cancer: a formal meta-analysis of comparative studies on recurrence and toxicity. J Urol 169(1): 90–5
Cho WJ, Kim TH, Lee HS, Chung JW, Lee HN, Lee KS (2013) Treatment of urethral/bladder neck stricture after high-intensity focused ultrasound for prostate cancer with holmium: yttriumaluminium- garnet laser. Int Neurourol J 17(1): 24–9
Continence Product Advisor (2018) Indwelling catheters. Available online: www.continenceproductadvisor.org/products/catheters/indwellingcatheters (last accessed 30 January, 2018)
Dingwall L, McLafferty E (2006) Nurses’ perceptions of indwelling urinary catheters in older people. Nurs Standard 21(14): 35–42
Diokno Ac, Sonda LP, Hollander JB, Lapides J (1983) Fate of patients started on clean intermittent selfcatheterisation therapy 10 years ago. J Urol 129(6): 1120–2
Doughty L, Lister S (2015) The Royal Marsden Manual of Clinical Nursing Procedures (Royal Marsden Manual Series). 9th edn. Elimination. Wiley- Blackwell, UK: chap 5
European Association of Urology Nurses (2013) Catheterisation: urethral intermittent in adults. Evidence-based Guidelines for Best Practice in Urological Health Care. EAUN. Available online: http://nurses.uroweb.org/guideline/catheterisation-urethral-intermittent-inadults (last accessed 30 January, 2018)
Feneley R, Hopley I, Wells P (2015) Urinary catheters: history, current status, adverse events and research agenda. J Med Eng Technol 39(8): 459–70
Fillingham S, Douglas J, eds (2004) Urological Nursing. 3rd edn. Baillière Tindall, UK
Igawa Y, Wyndaele JJ, Nishizawa O (2008) Catheterization: Possible complications and their prevention and treatment. Int J Urol (15): 481–5
Kim DY, Chancellor MB (2000) Intravesical neuromodulatory drugs: capsaicin and resiniferatoxin to treat the overactive bladder. J Endourol 14(1): 97–103
Lapides J, Diokno AC, Silber SM, Lowe BS (1972) Clean intermittent selfcatheterisation in the treatment of urinary tract disease. J Urol 107(3): 458–61
Lapides J, Diokno AC, Lowe BS, Kalish MD (1974) Follow-up on unsterile intermittent self-catheterisation. J Urol 111(2): 184–7
Lapides J, Diokno AC, Gould FR, Lowe BS (1976) Further observations on selfcatheterisation. J Urol 116(2): 169–71
Logan K, Shaw C, Webber I, Samuel S, Broome L (2008) Patients; experiences of learning clean intermittent selfcatheterisation: a qualitative study. J Adv Nurs 62(1): 32–40
Logan K (2017) The female experience of ISC with a silicone catheter. Br J Nurs 26(2): 82–8
Mangnall J (2013) Key considerations of intermittent self-catheterisation. Br J Nurs 21(7): 392–8
Robinson J (2006) Intermittent selfcatheterisation: principles and practice. Br J Community Nurs 11(4): 144–52
Roehrborn CG, Schwinn DA (2004) Alpha 1-adrenergic receptors and their inhibitors in lower urinary tract symptoms and benign prostatic hyperplasia. J Urol 171: 1029–35
Royal College of Nursing (2012) Catheter Care: RCN Guidance for Nurses. RCN, London
Shaw C, Logan K (2013) Psychological coping with intermittent selfcatheterisation( ISC) in people with spinal injury: a qualitative study. Int J Nurs Stud 50(10): 1341–50
Shaw C, Logan K, Webber I, Broome L, Samuel S (2008) Effect of clean intermittent self-catheterisation on quality of life: a qualitative study. J Adv Nurs 61(6): 641–50
Urology textbook (2018) Anatomy of the Bladder. Available online: www.urologytextbook.com/bladder-anatomy.html (last accessed 30 January, 2018)
Van Achterburg T, Holleman G, Cobussen-Boekhourst H, Arts R, Heesakkers J (2007) Adherence to clean intermittent catheterisation: determinants explored. J Clin Nurs 17(3): 394–402
Bardsley A (2015) ISC in women following urogynaecologic surgery. Br J Nurs (urology supplement) 20(18): S6–S13
Barton R (2000) Intermittent self catheterisation. Nurs Standard 15(9): 47–52
Bohle A, Jocham D, Bock PR (2003) Intravesical bacillus Calmette-Guerin versus mitomycin C for superficial bladder cancer: a formal meta-analysis of comparative studies on recurrence and toxicity. J Urol 169(1): 90–5
Cho WJ, Kim TH, Lee HS, Chung JW, Lee HN, Lee KS (2013) Treatment of urethral/bladder neck stricture after high-intensity focused ultrasound for prostate cancer with holmium: yttriumaluminium- garnet laser. Int Neurourol J 17(1): 24–9
Continence Product Advisor (2018) Indwelling catheters. Available online: www.continenceproductadvisor.org/products/catheters/indwellingcatheters (last accessed 30 January, 2018)
Dingwall L, McLafferty E (2006) Nurses’ perceptions of indwelling urinary catheters in older people. Nurs Standard 21(14): 35–42
Diokno Ac, Sonda LP, Hollander JB, Lapides J (1983) Fate of patients started on clean intermittent selfcatheterisation therapy 10 years ago. J Urol 129(6): 1120–2
Doughty L, Lister S (2015) The Royal Marsden Manual of Clinical Nursing Procedures (Royal Marsden Manual Series). 9th edn. Elimination. Wiley- Blackwell, UK: chap 5
European Association of Urology Nurses (2013) Catheterisation: urethral intermittent in adults. Evidence-based Guidelines for Best Practice in Urological Health Care. EAUN. Available online: http://nurses.uroweb.org/guideline/catheterisation-urethral-intermittent-inadults (last accessed 30 January, 2018)
Feneley R, Hopley I, Wells P (2015) Urinary catheters: history, current status, adverse events and research agenda. J Med Eng Technol 39(8): 459–70
Fillingham S, Douglas J, eds (2004) Urological Nursing. 3rd edn. Baillière Tindall, UK
Igawa Y, Wyndaele JJ, Nishizawa O (2008) Catheterization: Possible complications and their prevention and treatment. Int J Urol (15): 481–5
Kim DY, Chancellor MB (2000) Intravesical neuromodulatory drugs: capsaicin and resiniferatoxin to treat the overactive bladder. J Endourol 14(1): 97–103
Lapides J, Diokno AC, Silber SM, Lowe BS (1972) Clean intermittent selfcatheterisation in the treatment of urinary tract disease. J Urol 107(3): 458–61
Lapides J, Diokno AC, Lowe BS, Kalish MD (1974) Follow-up on unsterile intermittent self-catheterisation. J Urol 111(2): 184–7
Lapides J, Diokno AC, Gould FR, Lowe BS (1976) Further observations on selfcatheterisation. J Urol 116(2): 169–71
Logan K, Shaw C, Webber I, Samuel S, Broome L (2008) Patients; experiences of learning clean intermittent selfcatheterisation: a qualitative study. J Adv Nurs 62(1): 32–40
Logan K (2017) The female experience of ISC with a silicone catheter. Br J Nurs 26(2): 82–8
Mangnall J (2013) Key considerations of intermittent self-catheterisation. Br J Nurs 21(7): 392–8
Robinson J (2006) Intermittent selfcatheterisation: principles and practice. Br J Community Nurs 11(4): 144–52
Roehrborn CG, Schwinn DA (2004) Alpha 1-adrenergic receptors and their inhibitors in lower urinary tract symptoms and benign prostatic hyperplasia. J Urol 171: 1029–35
Royal College of Nursing (2012) Catheter Care: RCN Guidance for Nurses. RCN, London
Shaw C, Logan K (2013) Psychological coping with intermittent selfcatheterisation( ISC) in people with spinal injury: a qualitative study. Int J Nurs Stud 50(10): 1341–50
Shaw C, Logan K, Webber I, Broome L, Samuel S (2008) Effect of clean intermittent self-catheterisation on quality of life: a qualitative study. J Adv Nurs 61(6): 641–50
Urology textbook (2018) Anatomy of the Bladder. Available online: www.urologytextbook.com/bladder-anatomy.html (last accessed 30 January, 2018)
Van Achterburg T, Holleman G, Cobussen-Boekhourst H, Arts R, Heesakkers J (2007) Adherence to clean intermittent catheterisation: determinants explored. J Clin Nurs 17(3): 394–402