

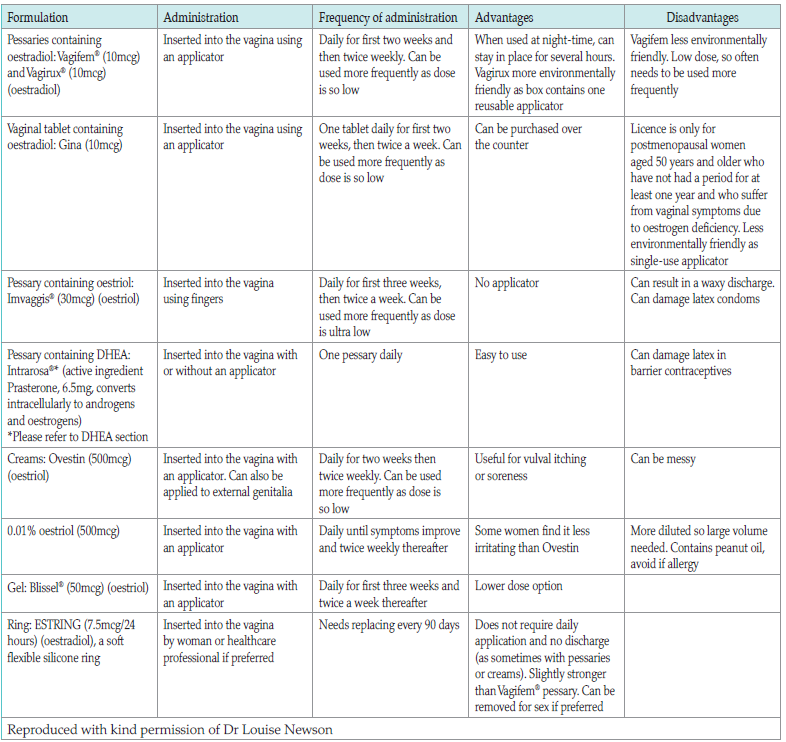
Table 1: Summary of localised hormonal treatments
References
American College of Obstetricians and Gynecologists (2016) ACOG Committee Opinion No. 659: The use of vaginal estrogen in women with a history of estrogen-dependent breast cancer. Obstet Gynecol 127(3): e93–e96. Reaffirmed 2020
Davis SR, Barber R, Panay N (2019) Global consensus position statement on the use of testosterone therapy for women. Climacteric 22: 429–34
Hillard T, Abernethy K, Hamoda H, et al (2017) Management of the Menopause. 6th edn. British Menopause Society
Hirschberg AL, Bitzer J, Cano A, et al (2021) Topical estrogens and nonhormonal preparations for postmenopausal vulvovaginal atrophy: an EMAS clinical guide. Maturitas 148: 55–61
Kearley-Shiers K, Holloway D, Rymer J, et al (2022) Intravaginal dehydroepiandrosterone for genitourinary symptoms of the menopause: Is the evidence sufficient? Post Reproductive Health 28(4): 237–43
Kim MM; Kreydin EI (2018) The association of serum testosterone levels and urinary incontinence in women. J Urol 199: 522–7
Laing AJ, Newson LN, Simon JA (2022) Individual benefits and risks of intravaginal estrogen and systemic testosterone in the management of women in the menopause, with a discussion of any associated risks for cancer development. Cancer J 28(3): 196–203
Martin DM, Kakumani S, Martin MS, Cassidy G (2003) Learning disabilities and the menopause. J Br Menopause Soc 9(1): 22–6
Nappi RE, Palacios S (2014) Impact of vulvovaginal atrophy on sexual health and quality of life at postmenopause. Climacteric 17(1): 3–9
Nappi RE, Kingsberg S, Maamari R, et al (2013) The CLOSER (Clarifying Vaginal Atrophy’s Impact On Sex and Relationships) survey: implications of vaginal discomfort in postmenopausal women and in male partners. J Sex Med 10(9): 2232–41
Nappi RE, Kokot-Kierepa M (2012) Vaginal Health: Insights, Views & Attitudes (VIVA) — results from an international survey. Climacteric 15(1): 36–44
National Institute for Health and Care Excellence (2015) Menopause: diagnosis and management. NICE guideline [NG23];[updated 2019, Dec]. Available online: www.nice.org.uk/guidance/ng23
Newson L, Kirby M, Stillwell S, et al (2021) Position statement for management of genitourinary syndrome of menopause. British Society for Sexual Medicine. Revised and updated in January 2023. Available online: https://balance-menopause.com/uploads/2021/10/GSM-BSSM-2023.pdf
Phillips C, Hillard T, Salvatore S, Cardozo L, Toozs-Hobson P (2022) on behalf of the Royal College of Obstetricians and Gynaecologists. Laser treatment for genitourinary syndrome of menopause. BJOG 129: e89–e94
Pitkin J, on behalf of the British Menopause Society medical advisory council (2018) BMS Consensus Statement: Urogenital atrophy. 2018. Available online: https://thebms.org.uk/publications/consensusstatements/urogenital-atrophy/
Pitsouni E, Grigoriadis T, Douskos A, et al (2018) Efficacy of vaginal therapies alternative to vaginal estrogens on sexual function and orgasm of menopausal women: a systematic review and metanalysis of randomized controlled trials. Eur J Obstet Gynecol Reprod Biol 229: 45–56
Portman DJ, Gass MLS (2014) Vulvovaginal Atrophy Terminology Consensus Conference Panel. Genitourinary syndrome of menopause: New terminology for vulvovaginal atrophy from the International Society for the Study of Women’s Sexual Health and the North American Menopause Society. Menopause. J North Am Menopause Soc 21(10): 1063–68
Santen RJ, Pinkerton JV, Liu JH, et al (2019) Symposium report. Workshop on normal reference ranges for estradiol in postmenopausal women. Menopause 27: 614–24
Stuenkel CA, Davis SR, Gompel A, et al (2015) Treatment of symptoms of the menopause: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 100(11): 3975–4011
Sturdee DW, Panay N (2010) IMS Writing Group. Recommendations for the management of postmenopausal vaginal atrophy. Climacteric 13(6): 509–22
Women’s Health Concern (2022) Urogenital Problems. Factsheet. Available online: www.womens-health-concern.org/wp-content/uploads/2022/12/23-WHC-FACTSHEET-UrogenitalProblems-NOV2022-B.pdf
Davis SR, Barber R, Panay N (2019) Global consensus position statement on the use of testosterone therapy for women. Climacteric 22: 429–34
Hillard T, Abernethy K, Hamoda H, et al (2017) Management of the Menopause. 6th edn. British Menopause Society
Hirschberg AL, Bitzer J, Cano A, et al (2021) Topical estrogens and nonhormonal preparations for postmenopausal vulvovaginal atrophy: an EMAS clinical guide. Maturitas 148: 55–61
Kearley-Shiers K, Holloway D, Rymer J, et al (2022) Intravaginal dehydroepiandrosterone for genitourinary symptoms of the menopause: Is the evidence sufficient? Post Reproductive Health 28(4): 237–43
Kim MM; Kreydin EI (2018) The association of serum testosterone levels and urinary incontinence in women. J Urol 199: 522–7
Laing AJ, Newson LN, Simon JA (2022) Individual benefits and risks of intravaginal estrogen and systemic testosterone in the management of women in the menopause, with a discussion of any associated risks for cancer development. Cancer J 28(3): 196–203
Martin DM, Kakumani S, Martin MS, Cassidy G (2003) Learning disabilities and the menopause. J Br Menopause Soc 9(1): 22–6
Nappi RE, Palacios S (2014) Impact of vulvovaginal atrophy on sexual health and quality of life at postmenopause. Climacteric 17(1): 3–9
Nappi RE, Kingsberg S, Maamari R, et al (2013) The CLOSER (Clarifying Vaginal Atrophy’s Impact On Sex and Relationships) survey: implications of vaginal discomfort in postmenopausal women and in male partners. J Sex Med 10(9): 2232–41
Nappi RE, Kokot-Kierepa M (2012) Vaginal Health: Insights, Views & Attitudes (VIVA) — results from an international survey. Climacteric 15(1): 36–44
National Institute for Health and Care Excellence (2015) Menopause: diagnosis and management. NICE guideline [NG23];[updated 2019, Dec]. Available online: www.nice.org.uk/guidance/ng23
Newson L, Kirby M, Stillwell S, et al (2021) Position statement for management of genitourinary syndrome of menopause. British Society for Sexual Medicine. Revised and updated in January 2023. Available online: https://balance-menopause.com/uploads/2021/10/GSM-BSSM-2023.pdf
Phillips C, Hillard T, Salvatore S, Cardozo L, Toozs-Hobson P (2022) on behalf of the Royal College of Obstetricians and Gynaecologists. Laser treatment for genitourinary syndrome of menopause. BJOG 129: e89–e94
Pitkin J, on behalf of the British Menopause Society medical advisory council (2018) BMS Consensus Statement: Urogenital atrophy. 2018. Available online: https://thebms.org.uk/publications/consensusstatements/urogenital-atrophy/
Pitsouni E, Grigoriadis T, Douskos A, et al (2018) Efficacy of vaginal therapies alternative to vaginal estrogens on sexual function and orgasm of menopausal women: a systematic review and metanalysis of randomized controlled trials. Eur J Obstet Gynecol Reprod Biol 229: 45–56
Portman DJ, Gass MLS (2014) Vulvovaginal Atrophy Terminology Consensus Conference Panel. Genitourinary syndrome of menopause: New terminology for vulvovaginal atrophy from the International Society for the Study of Women’s Sexual Health and the North American Menopause Society. Menopause. J North Am Menopause Soc 21(10): 1063–68
Santen RJ, Pinkerton JV, Liu JH, et al (2019) Symposium report. Workshop on normal reference ranges for estradiol in postmenopausal women. Menopause 27: 614–24
Stuenkel CA, Davis SR, Gompel A, et al (2015) Treatment of symptoms of the menopause: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 100(11): 3975–4011
Sturdee DW, Panay N (2010) IMS Writing Group. Recommendations for the management of postmenopausal vaginal atrophy. Climacteric 13(6): 509–22
Women’s Health Concern (2022) Urogenital Problems. Factsheet. Available online: www.womens-health-concern.org/wp-content/uploads/2022/12/23-WHC-FACTSHEET-UrogenitalProblems-NOV2022-B.pdf