

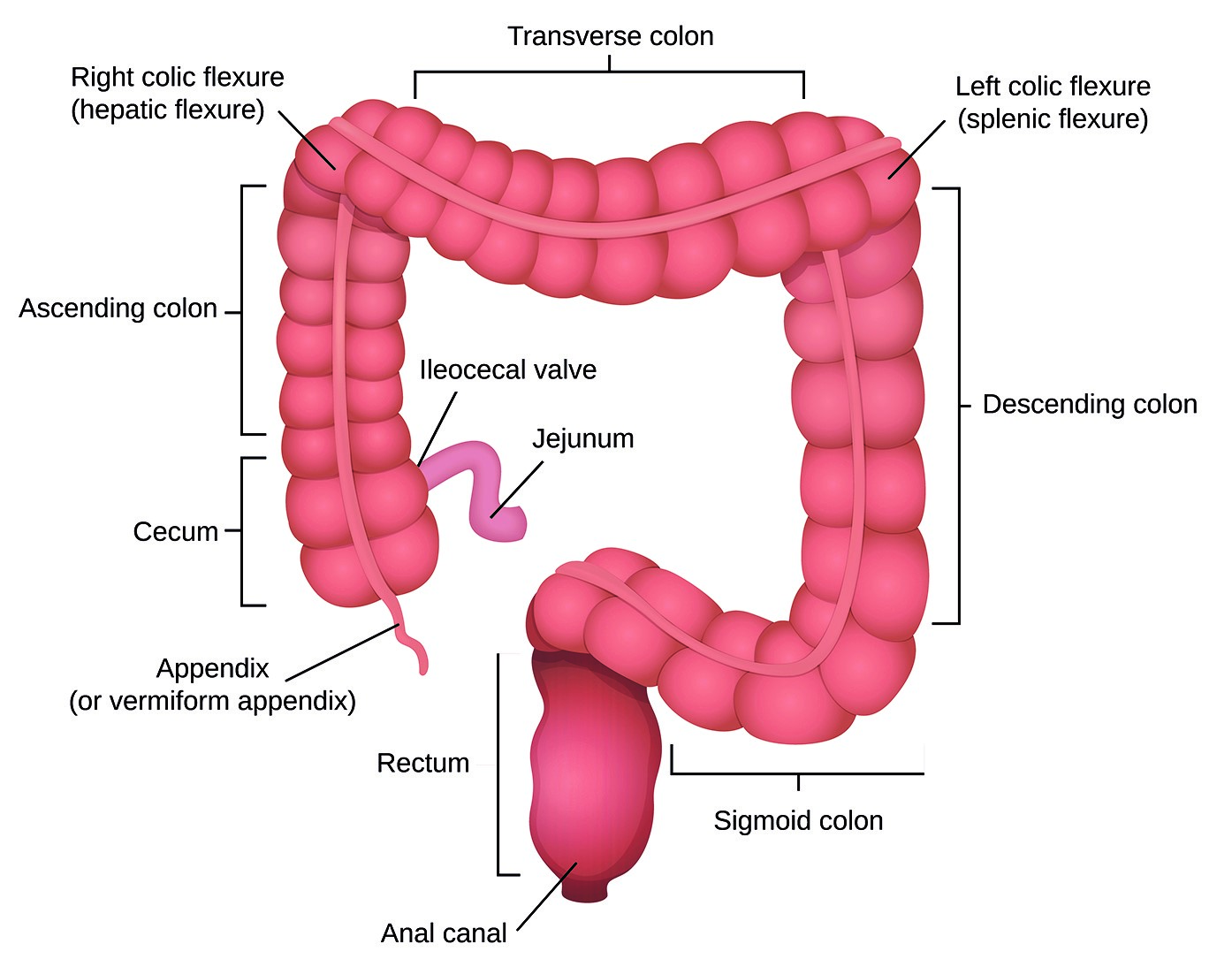
Figure 1. Anatomy of the large intestine.
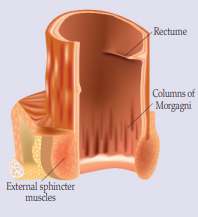
Figure 2. Rectum and internal and external sphincters.
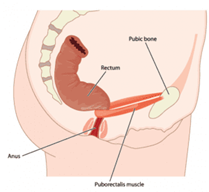
Figure 3. Puborectalis muscle contracted.
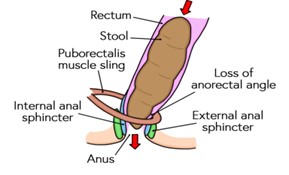
Figure 4. Puborectalis muscle at rest to allow passage of stool.
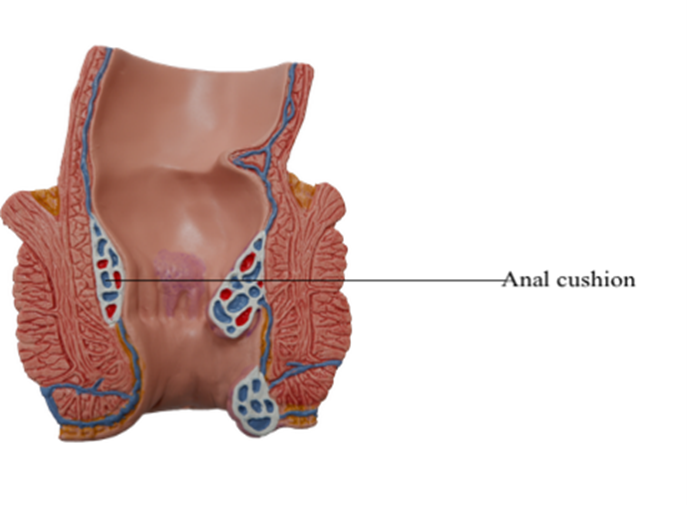
Figure 5. Anal cushions.
References
Assmann SL, Keszthelyi D, Kleijnen J, et al (2022) Guideline for the diagnosis and treatment of Faecal Incontinence – A UEG/ESCP/ESNM/ESPCG collaboration. United European Gastroenterol J 10(3): 251-86
Benezech A, Bouvier M, Vitton V (2016) Faecal incontinence: current knowledges and perspectives. World J Gastrointest Pathophysiol 7(1): 59-71
Bliss DZ, Mimura T, Berghmans B, et al (2017) Assessment and conservative management of faecal incontinence and quality of life in adults. In: Abrams P, Cardozo L, Wagg A, Wein A, editors. Incontinence. 6th ed. International Continence Society, Bristol
Camilleri-Brennan J (2020) Introductory chapter. Challenges in the diagnosis and treatment of faecal incontinence. In: Current Topics in Faecal Incontinence. IntechOpen. Available online: https://www.researchgate.net/publication/341185132_Introductory_Chapter_Challenges_in_the_Diagnosis_and_Treatment_of_Faecal_Incontinence
Duelund-Jakobsen J, Worsoe J, Lundby L, Christensen P, Krough K (2016) Management of patients with faecal incontinence. Therap Adv Gastroenterol 9(1): 86-97
Harari D (2009) Faecal incontinence in older people. Rev Clin Gerontol 19(2): 87-101
International Continence Society (ICS) (2015) Fact Sheets. A Background to Urinary and Faecal Incontinence. Available online: https://www.ics.org/folder/82
National Institute of Clinical Excellence (NICE) (2014) Faecal incontinence in adults. Quality Standard 54. Available online: www.nice.org.uk/guidance/qs54
Norton C, Chelvanayagam S (2004) Bowel continence Nursing. Beaconsfield Publishers Ltd, Beaconsfield
Norton C, Whitehead WE, Bliss DZ, Harari D, Lang J (2010) Management of faecal incontinence in adults. Neurourol Urodyn 29(1): 199-206
Potter J, Peel P, Main S, et al (2007) National audit of continence care for older people: management of faecal incontinence. Age Ageing 36(3): 268-73
Royal College of Nursing (2019) Bowel care. Management of lower bowel dysfunction, including digital rectal examination and digital removal of faeces. Available online: https://www.rcn.org.uk/professional-development/publications/pub-007522
Salvatore S, Delancey J, Igawa Y, et al (2017) Pathophysiology of Urinary incontinence, Faecal Incontinence and Pelvic organ prolapse. In: Incontinence 6th edition. (Eds) Abrams P, Cardozo L, Wagg A, Wein A. ICUD ICS, Tokyo
Sbeit W, Khoury T, Mari A (2021) Diagnostic approach to faecal incontinence: what test and when to perform? World J Gastroenterol 27(15): 1553-62
Young J (2022) Assessment and management of faecal incontinence. J Community Nurs 36(2): 51–8
Benezech A, Bouvier M, Vitton V (2016) Faecal incontinence: current knowledges and perspectives. World J Gastrointest Pathophysiol 7(1): 59-71
Bliss DZ, Mimura T, Berghmans B, et al (2017) Assessment and conservative management of faecal incontinence and quality of life in adults. In: Abrams P, Cardozo L, Wagg A, Wein A, editors. Incontinence. 6th ed. International Continence Society, Bristol
Camilleri-Brennan J (2020) Introductory chapter. Challenges in the diagnosis and treatment of faecal incontinence. In: Current Topics in Faecal Incontinence. IntechOpen. Available online: https://www.researchgate.net/publication/341185132_Introductory_Chapter_Challenges_in_the_Diagnosis_and_Treatment_of_Faecal_Incontinence
Duelund-Jakobsen J, Worsoe J, Lundby L, Christensen P, Krough K (2016) Management of patients with faecal incontinence. Therap Adv Gastroenterol 9(1): 86-97
Harari D (2009) Faecal incontinence in older people. Rev Clin Gerontol 19(2): 87-101
International Continence Society (ICS) (2015) Fact Sheets. A Background to Urinary and Faecal Incontinence. Available online: https://www.ics.org/folder/82
National Institute of Clinical Excellence (NICE) (2014) Faecal incontinence in adults. Quality Standard 54. Available online: www.nice.org.uk/guidance/qs54
Norton C, Chelvanayagam S (2004) Bowel continence Nursing. Beaconsfield Publishers Ltd, Beaconsfield
Norton C, Whitehead WE, Bliss DZ, Harari D, Lang J (2010) Management of faecal incontinence in adults. Neurourol Urodyn 29(1): 199-206
Potter J, Peel P, Main S, et al (2007) National audit of continence care for older people: management of faecal incontinence. Age Ageing 36(3): 268-73
Royal College of Nursing (2019) Bowel care. Management of lower bowel dysfunction, including digital rectal examination and digital removal of faeces. Available online: https://www.rcn.org.uk/professional-development/publications/pub-007522
Salvatore S, Delancey J, Igawa Y, et al (2017) Pathophysiology of Urinary incontinence, Faecal Incontinence and Pelvic organ prolapse. In: Incontinence 6th edition. (Eds) Abrams P, Cardozo L, Wagg A, Wein A. ICUD ICS, Tokyo
Sbeit W, Khoury T, Mari A (2021) Diagnostic approach to faecal incontinence: what test and when to perform? World J Gastroenterol 27(15): 1553-62
Young J (2022) Assessment and management of faecal incontinence. J Community Nurs 36(2): 51–8