


Table 1: Causes of chronic cough (adapted from NHS Inform Scotland, 2023a; Mayo Clinic, 2019).
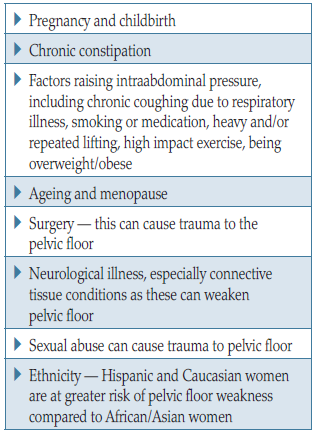
Table 2: Pelvic floor weakness — risk factors (Abrams et al, 2017; Yates, 2019a).
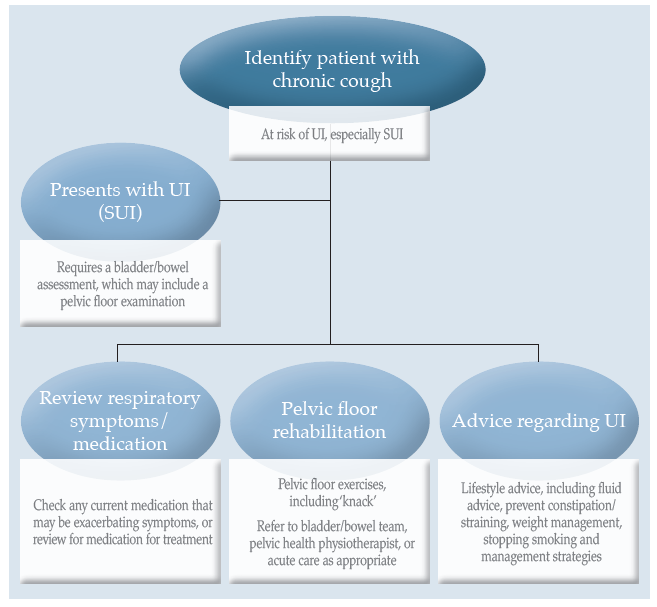
Figure 1. Sample flow chart to indicate pathway for individuals with chronic cough presenting with UI.
References
Abram P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, et al (2010) The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn 29: 213–40
Abrams P, Cardozo L, Wagg A, Wein A, eds (2017) Incontinence. International Continence Society, Bristol
Barrie M (2018) Respiratory conditions and urinary incontinence. J Community Nurs 32(1): 20–6
Battaglia S, Benfante A, Principe S, Basile L, Scichilone N (2019) Urinary incontinence in chronic obstructive pulmonary disease: a common co-morbidity or a typical adverse effect. Drugs Aging 36(9): 799–806
Burge AT, Lee AL, Kein C, Button BM, Sherburn MS, Miller B, Holland AE (2017) Prevalence and impact of urinary incontinence in men with chronic obstructive pulmonary disease: a questionnaire survey. J Physiother 103: 53–8
Button BM, Holland AE, Sherburn MS, Chase J, Wilson JW, Burge AT (2019) Prevalence, impact and specialised treatment of urinary incontinence in women with chronic lung disease. Physiotherapy 105: 114–19
Çolak Y, Nordestgaard BG, Laursen LC, Afzal S, Lange P, Dahl M (2017) Risk factors for chronic cough among 14,669 individuals from the general population. Chest 152(3): 563–73
Colley W (2020) Colley Model. Supporting the assessment of bladder symptoms in adults. Available online: www.continenceassessment.co.uk
Dorey G (2003) Clench it or drench it! A self-help guide for ladies who lunch, laugh and leak. Grace Dorey, Barnstaple
Haukeland-Parker S, Frisk B, Spruit MA, Stafne SN, Johannessen HH (2021) Treatment of urinary incontinence in women with chronic obstructive pulmonary disease – a randomised controlled study. Trials 22(1): 900
Haylen BT, de Ridder D, Freeman RM, Swift SE, Berghmans B, Lee J, et al (2010) An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol 29: 4–20
Hennessey S (2023) A urinary incontinence service for patients with chronic cough. Nurs Times 119: 4
Hongmei D, Cuiqui S, Xianghuai X, Li Y (2020) Drug-induced chronic cough and the possible mechanism of action. Ann Palliat Med 9(5): 3562–70
Mayo Clinic (2019) Chronic cough – symptoms and causes. Available online: www.mayoclinic.org>syc-20351575
NHS Inform Scotland (2023a) Cough. Available online: www.nhsinform.scot/illness-and-conditions/lung-and-airways/cough
NHS Inform Scotland (2023b) Why does COPD happen? Available online: www.nhsinform.scot/illness-and-conditions/lung-and-airways/copd/chronic-obstructive-pulmonary–disease
Pelvic Obstetric and Gynaecological Physiotherapy (2018) The Pelvic Floor Muscles: A Guide for Women. Available online: https://pogp.csp.org.uk/publications/pelvic-floor-muscle-exercise-women
Salman Q, Majeed R, Shafee I, Arif S, Waris M, Ayyub A (2022) Frequency of stress urinary incontinence with chronic obstructive pulmonary disease in men; a cross sectional survey. Multicultural Education 8(12): 110–14
Yang C, Feng Z, Chen Z, et al (2022) The risk factors for urinary incontinence in female adults with chronic cough. BMC Pulm Med 22(1): 276
Yates A (2019a) Female pelvic floor 1: anatomy and pathophysiology. Nurs Times 115(5): 18–21
Yates A (2019b) Basic continence assessment: what community nurses should know. J Community Nurs 33(3): 52–5
Yates A (2019c) Female pelvic floor 2: assessment and rehabilitation. Nurs Times 115(6): 30–3
Abrams P, Cardozo L, Wagg A, Wein A, eds (2017) Incontinence. International Continence Society, Bristol
Barrie M (2018) Respiratory conditions and urinary incontinence. J Community Nurs 32(1): 20–6
Battaglia S, Benfante A, Principe S, Basile L, Scichilone N (2019) Urinary incontinence in chronic obstructive pulmonary disease: a common co-morbidity or a typical adverse effect. Drugs Aging 36(9): 799–806
Burge AT, Lee AL, Kein C, Button BM, Sherburn MS, Miller B, Holland AE (2017) Prevalence and impact of urinary incontinence in men with chronic obstructive pulmonary disease: a questionnaire survey. J Physiother 103: 53–8
Button BM, Holland AE, Sherburn MS, Chase J, Wilson JW, Burge AT (2019) Prevalence, impact and specialised treatment of urinary incontinence in women with chronic lung disease. Physiotherapy 105: 114–19
Çolak Y, Nordestgaard BG, Laursen LC, Afzal S, Lange P, Dahl M (2017) Risk factors for chronic cough among 14,669 individuals from the general population. Chest 152(3): 563–73
Colley W (2020) Colley Model. Supporting the assessment of bladder symptoms in adults. Available online: www.continenceassessment.co.uk
Dorey G (2003) Clench it or drench it! A self-help guide for ladies who lunch, laugh and leak. Grace Dorey, Barnstaple
Haukeland-Parker S, Frisk B, Spruit MA, Stafne SN, Johannessen HH (2021) Treatment of urinary incontinence in women with chronic obstructive pulmonary disease – a randomised controlled study. Trials 22(1): 900
Haylen BT, de Ridder D, Freeman RM, Swift SE, Berghmans B, Lee J, et al (2010) An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol 29: 4–20
Hennessey S (2023) A urinary incontinence service for patients with chronic cough. Nurs Times 119: 4
Hongmei D, Cuiqui S, Xianghuai X, Li Y (2020) Drug-induced chronic cough and the possible mechanism of action. Ann Palliat Med 9(5): 3562–70
Mayo Clinic (2019) Chronic cough – symptoms and causes. Available online: www.mayoclinic.org>syc-20351575
NHS Inform Scotland (2023a) Cough. Available online: www.nhsinform.scot/illness-and-conditions/lung-and-airways/cough
NHS Inform Scotland (2023b) Why does COPD happen? Available online: www.nhsinform.scot/illness-and-conditions/lung-and-airways/copd/chronic-obstructive-pulmonary–disease
Pelvic Obstetric and Gynaecological Physiotherapy (2018) The Pelvic Floor Muscles: A Guide for Women. Available online: https://pogp.csp.org.uk/publications/pelvic-floor-muscle-exercise-women
Salman Q, Majeed R, Shafee I, Arif S, Waris M, Ayyub A (2022) Frequency of stress urinary incontinence with chronic obstructive pulmonary disease in men; a cross sectional survey. Multicultural Education 8(12): 110–14
Yang C, Feng Z, Chen Z, et al (2022) The risk factors for urinary incontinence in female adults with chronic cough. BMC Pulm Med 22(1): 276
Yates A (2019a) Female pelvic floor 1: anatomy and pathophysiology. Nurs Times 115(5): 18–21
Yates A (2019b) Basic continence assessment: what community nurses should know. J Community Nurs 33(3): 52–5
Yates A (2019c) Female pelvic floor 2: assessment and rehabilitation. Nurs Times 115(6): 30–3