

QUALITY OF LIFE
The consequences of nocturia are varied and numerous. The condition is associated with an increased incidence of falls and fractures – especially hip fractures – and an increased fear of falling (Varilla et al, 2011). Falling is due to elderly people getting out of bed in the dark to walk to the bathroom to void. As patients’ sleep is disturbed and fragmented due to the need to void at night, they can become drowsy during the day. This can increase fatigue and reduce energy levels; impair balance, perception, concentration and memory; lower mood; and cause depression (Varilla et al, 2011). In turn, this can result in complications associated with immobility and debility, such as, pressure ulceration, malnutrition and increased risk of infection.The impact of nocturia on quality of life is comparable to the effects of other conditions, such as gout, hypertension, diabetes and angina. It also affects an individual’s perception of their age (i.e. people with nocturia feel older), as well as contributing to obesity and higher rates of death in patients with coronary heart disease. Nocturia can also lead to relationship disturbances or breakdown and increased admission to care homes (Varilla et al, 2011).
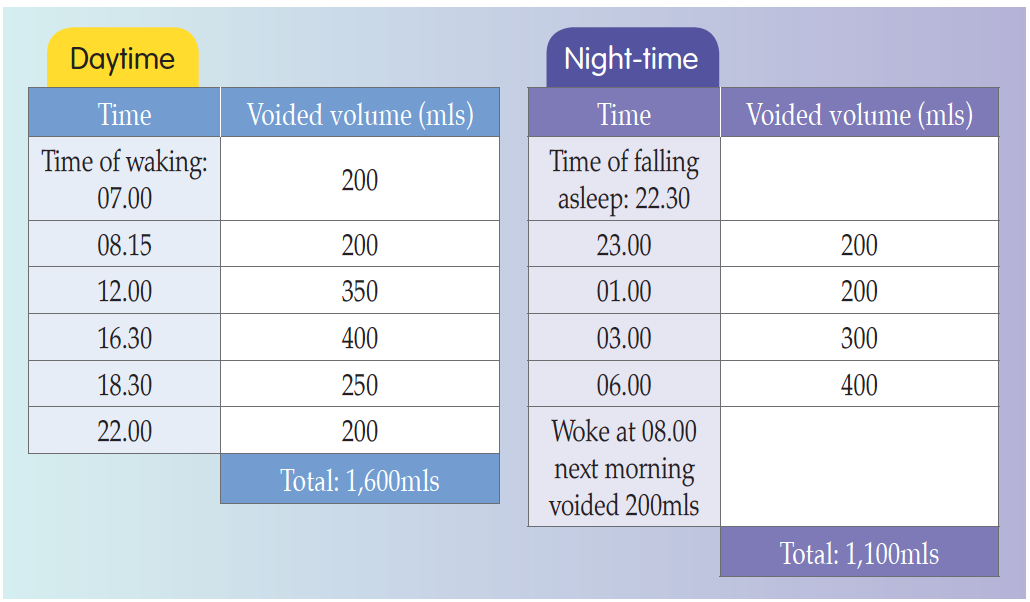 Figure 1.
Figure 1.Example of a frequency volume chart (FVC) (Hashim et al, 2019).
References
Doorn BV, Bosch JLHR (2012) Nocturia in older men. Maturitas 71: 8–12
Emmanuel A (2004) Constipation. In: Norton C, Chelvanayagam S, eds. Bowel Continence Nursing. Beaconsfield, Beaconsfield Publishers Ltd
Hashim H, Blanker MH, Drake MJ, et al (2019) International Continence Society (ICS) report on the terminology for nocturia and nocturnal lower urinary tract function. Neurourol Urodyn 38(2): 499–508
Johnson TM (2017) Nocturia: clinical presentation, diagnosis, and treatment. Available online: www.uptodate.com/contents/nocturia-clinical-presentationdaignosis-and-treatment
Kujubu DA, Aboseif SR (2007) Evaluation of nocturia in the elderly. Perm J 11(1): 37–9
Oelke M, De Wachter S, Drake MJ, et al (2017) A practical approach to the management of nocturia. Int J Clin Pract 71: e13027
Prince D, Pedler K, Rashid P (2012) Nocturia — a guide to assessment and management. Aust Fam Physician 41(6): 399–402
Van Kerrebroeck P, Abrams P, Chaikin D, et al (2002) The standardisation of terminology in nocturia: report from the standardisation sub-committee of the International Continence Society. Neurourol Urodyn 21(2): 179–83
Varilla V, Samala RV, Galindo D, Ciocon J (2011) Nocturia in the elderly: a wake-up call. Cleve Clin J Med 78(11): 757–64
Yates A (2017) Nocturia in older people living in residential care. Nurs Res Care 19(11): 616–18
Emmanuel A (2004) Constipation. In: Norton C, Chelvanayagam S, eds. Bowel Continence Nursing. Beaconsfield, Beaconsfield Publishers Ltd
Hashim H, Blanker MH, Drake MJ, et al (2019) International Continence Society (ICS) report on the terminology for nocturia and nocturnal lower urinary tract function. Neurourol Urodyn 38(2): 499–508
Johnson TM (2017) Nocturia: clinical presentation, diagnosis, and treatment. Available online: www.uptodate.com/contents/nocturia-clinical-presentationdaignosis-and-treatment
Kujubu DA, Aboseif SR (2007) Evaluation of nocturia in the elderly. Perm J 11(1): 37–9
Oelke M, De Wachter S, Drake MJ, et al (2017) A practical approach to the management of nocturia. Int J Clin Pract 71: e13027
Prince D, Pedler K, Rashid P (2012) Nocturia — a guide to assessment and management. Aust Fam Physician 41(6): 399–402
Van Kerrebroeck P, Abrams P, Chaikin D, et al (2002) The standardisation of terminology in nocturia: report from the standardisation sub-committee of the International Continence Society. Neurourol Urodyn 21(2): 179–83
Varilla V, Samala RV, Galindo D, Ciocon J (2011) Nocturia in the elderly: a wake-up call. Cleve Clin J Med 78(11): 757–64
Yates A (2017) Nocturia in older people living in residential care. Nurs Res Care 19(11): 616–18