


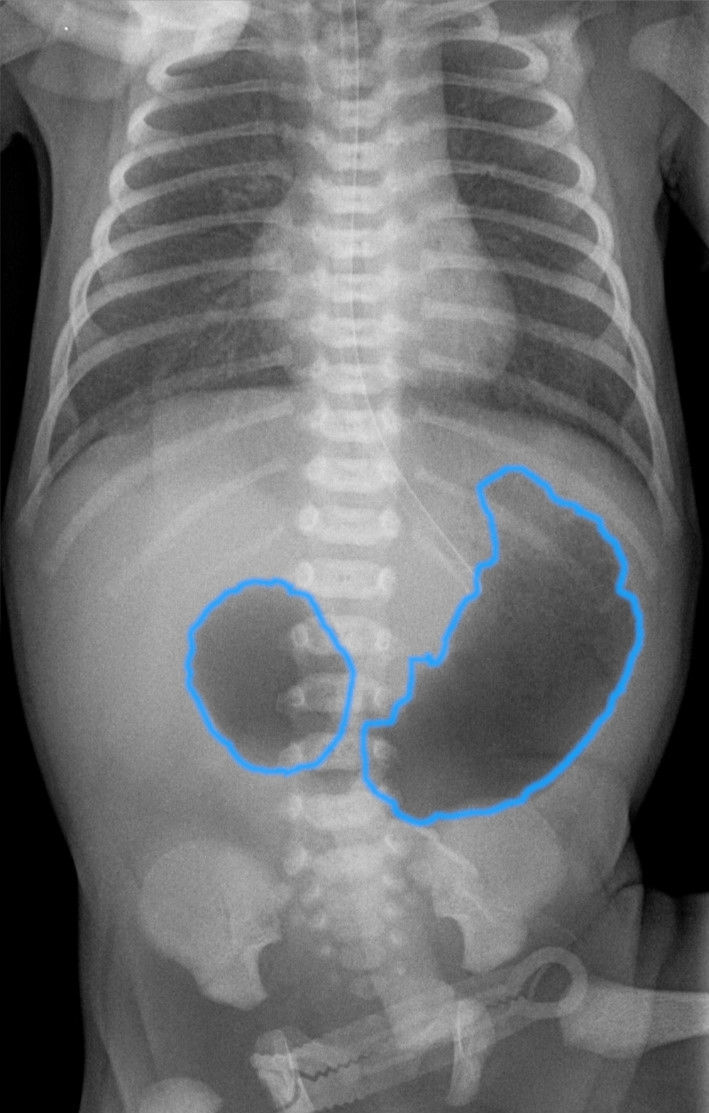
Figure 1. Double-bubble sign in a patient with duodenal atresia.

Figure 2. Abdominal X-ray showing Hirschsprung’s disease.
References
Atiyat DK, Al-Nusair DA, Alhajahjeh A, Al-Awadi MY, Aborajooh E (2025) Global prevalence of duodenal atresia in trisomy 21: a systematic review and meta-analysis. Eur J Pediatr Surg. 35(3):208-218. https://doi.org/10.1055/a-2471-6435
Bethell GS, Long AM, Knight M, Hall NJ; BAPS-CASS (2020) The impact of trisomy 21 on epidemiology, management, and outcomes of congenital duodenal obstruction: a population-based study. Pediatr Surg Int. 36(4):477-483. https://doi.org/10.1007/s00383-020-04628-w
Ciciora SL, Manickam K, Saps M (2023) Disorders of gut-brain interaction in a national cohort of children with Down syndrome. J Neurogastroenterol Motil. 29(1):94-101. https://doi.org/10.5056/jnm22055
Friedmacher F, Puri P (2013) Hirschsprung's disease associated with Down syndrome: a meta-analysis of incidence, functional outcomes and mortality. Pediatr Surg Int. 29(9):937-46. https://doi.org/10.1007/s00383-013-3361-1
Gely Y, Moreci R, Roberts H, Danos D, Zagory J (2025) Trisomy 21 children with duodenal atresia or anorectal malformation: NSQIP-P Surgical Outcomes Study. J Surg Res. 310:194-202. https://doi.org/10.1016/j.jss.2025.03.020
Gomes DOVS, Morais MB (2019) Gut microbiota and the use of probiotics in constipation in children and adolescents: systematic review. Rev Paul Pediatr. 38:e2018123. https://doi.org/10.1590/1984-0462/2020/38/2018123
Hom B, Boyd NK, Vogel BN et al (2024) Down syndrome and autoimmune disease. Clin Rev Allergy Immunol. 66(3):261-273. https://doi.org/10.1007/s12016-024-08996-2
Husby S, Koletzko S, Korponay-Szabó IR et al; ESPGHAN Working Group on Coeliac Disease Diagnosis; ESPGHAN Gastroenterology Committee; European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (2012) European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. 54(1):136-60. https://doi.org/10.1097/MPG.0b013e31821a23d0
Kenny SE, Tam PK, Garcia-Barcelo M (2010) Hirschsprung's disease. Semin Pediatr Surg. 19(3):194-200. https://doi.org/10.1053/j.sempedsurg.2010.03.004
Kwiatkowska M, Krogulska A (2021) The significance of the gut microbiome in children with functional constipation. Adv Clin Exp Med. 30(4):471-480. https://doi.org/10.17219/acem/131215
Mårild K, Stephansson O, Grahnquist L, Cnattingius S, Söderman G, Ludvigsson JF (2013) Down syndrome is associated with elevated risk of celiac disease: a nationwide case-control study. J Pediatr. 163(1):237-42. https://doi.org/10.1016/j.jpeds.2012.12.087
Martinelli M, Staiano A (2011) Motility problems in the intellectually challenged child, adolescent, and young adult. Gastroenterol Clin North Am. 40(4):765-75, viii. https://doi.org/10.1016/j.gtc.2011.09.009
Mishra D, Sehgal G, Verma RK, Rani A (2020) Association of trisomy 21 with anorectal malformation: a cytogenetic study. International Journal of Research in Medical Sciences. 8(5):1808–1812. https://doi.org/10.18203/2320-6012.ijrms20201932
Moore SW (2008) Down syndrome and the enteric nervous system. Pediatr Surg Int. 24(8):873-83. https://doi.org/10.1007/s00383-008-2188-7
Moras P, Zarfati A, Bagolan P, Conforti A, Toscano A, Iacobelli BD (2024) Anorectal malformations (ARM) and VACTERL association and severity of congenital heart diseases (CHD): Experience of 396 consecutive patients in a tertiary center. Pediatr Neonatol. 65(4):381-385. https://doi.org/10.1016/j.pedneo.2023.08.011
NHS England (2023) Constipation resources for people with a learning disability https://www.england.nhs.uk/publication/constipation-resources-for-people-with-a-learning-disability/ (accessed 29 January 2026)
Schill EM, Wright CM, Jamil A, LaCombe JM, Roper RJ, Heuckeroth RO (2019) Down syndrome mouse models have an abnormal enteric nervous system. JCI Insight. 5(11):e124510. https://doi.org/10.1172/jci.insight.124510
Travassos D, van Herwaarden-Lindeboom M, van der Zee DC (2011) Hirschsprung's disease in children with Down syndrome: a comparative study. Eur J Pediatr Surg. 21(4):220-3. https://doi.org/10.1055/s-0031-1271735
Bethell GS, Long AM, Knight M, Hall NJ; BAPS-CASS (2020) The impact of trisomy 21 on epidemiology, management, and outcomes of congenital duodenal obstruction: a population-based study. Pediatr Surg Int. 36(4):477-483. https://doi.org/10.1007/s00383-020-04628-w
Ciciora SL, Manickam K, Saps M (2023) Disorders of gut-brain interaction in a national cohort of children with Down syndrome. J Neurogastroenterol Motil. 29(1):94-101. https://doi.org/10.5056/jnm22055
Friedmacher F, Puri P (2013) Hirschsprung's disease associated with Down syndrome: a meta-analysis of incidence, functional outcomes and mortality. Pediatr Surg Int. 29(9):937-46. https://doi.org/10.1007/s00383-013-3361-1
Gely Y, Moreci R, Roberts H, Danos D, Zagory J (2025) Trisomy 21 children with duodenal atresia or anorectal malformation: NSQIP-P Surgical Outcomes Study. J Surg Res. 310:194-202. https://doi.org/10.1016/j.jss.2025.03.020
Gomes DOVS, Morais MB (2019) Gut microbiota and the use of probiotics in constipation in children and adolescents: systematic review. Rev Paul Pediatr. 38:e2018123. https://doi.org/10.1590/1984-0462/2020/38/2018123
Hom B, Boyd NK, Vogel BN et al (2024) Down syndrome and autoimmune disease. Clin Rev Allergy Immunol. 66(3):261-273. https://doi.org/10.1007/s12016-024-08996-2
Husby S, Koletzko S, Korponay-Szabó IR et al; ESPGHAN Working Group on Coeliac Disease Diagnosis; ESPGHAN Gastroenterology Committee; European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (2012) European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. 54(1):136-60. https://doi.org/10.1097/MPG.0b013e31821a23d0
Kenny SE, Tam PK, Garcia-Barcelo M (2010) Hirschsprung's disease. Semin Pediatr Surg. 19(3):194-200. https://doi.org/10.1053/j.sempedsurg.2010.03.004
Kwiatkowska M, Krogulska A (2021) The significance of the gut microbiome in children with functional constipation. Adv Clin Exp Med. 30(4):471-480. https://doi.org/10.17219/acem/131215
Mårild K, Stephansson O, Grahnquist L, Cnattingius S, Söderman G, Ludvigsson JF (2013) Down syndrome is associated with elevated risk of celiac disease: a nationwide case-control study. J Pediatr. 163(1):237-42. https://doi.org/10.1016/j.jpeds.2012.12.087
Martinelli M, Staiano A (2011) Motility problems in the intellectually challenged child, adolescent, and young adult. Gastroenterol Clin North Am. 40(4):765-75, viii. https://doi.org/10.1016/j.gtc.2011.09.009
Mishra D, Sehgal G, Verma RK, Rani A (2020) Association of trisomy 21 with anorectal malformation: a cytogenetic study. International Journal of Research in Medical Sciences. 8(5):1808–1812. https://doi.org/10.18203/2320-6012.ijrms20201932
Moore SW (2008) Down syndrome and the enteric nervous system. Pediatr Surg Int. 24(8):873-83. https://doi.org/10.1007/s00383-008-2188-7
Moras P, Zarfati A, Bagolan P, Conforti A, Toscano A, Iacobelli BD (2024) Anorectal malformations (ARM) and VACTERL association and severity of congenital heart diseases (CHD): Experience of 396 consecutive patients in a tertiary center. Pediatr Neonatol. 65(4):381-385. https://doi.org/10.1016/j.pedneo.2023.08.011
NHS England (2023) Constipation resources for people with a learning disability https://www.england.nhs.uk/publication/constipation-resources-for-people-with-a-learning-disability/ (accessed 29 January 2026)
Schill EM, Wright CM, Jamil A, LaCombe JM, Roper RJ, Heuckeroth RO (2019) Down syndrome mouse models have an abnormal enteric nervous system. JCI Insight. 5(11):e124510. https://doi.org/10.1172/jci.insight.124510
Travassos D, van Herwaarden-Lindeboom M, van der Zee DC (2011) Hirschsprung's disease in children with Down syndrome: a comparative study. Eur J Pediatr Surg. 21(4):220-3. https://doi.org/10.1055/s-0031-1271735